Case Report
Abstract
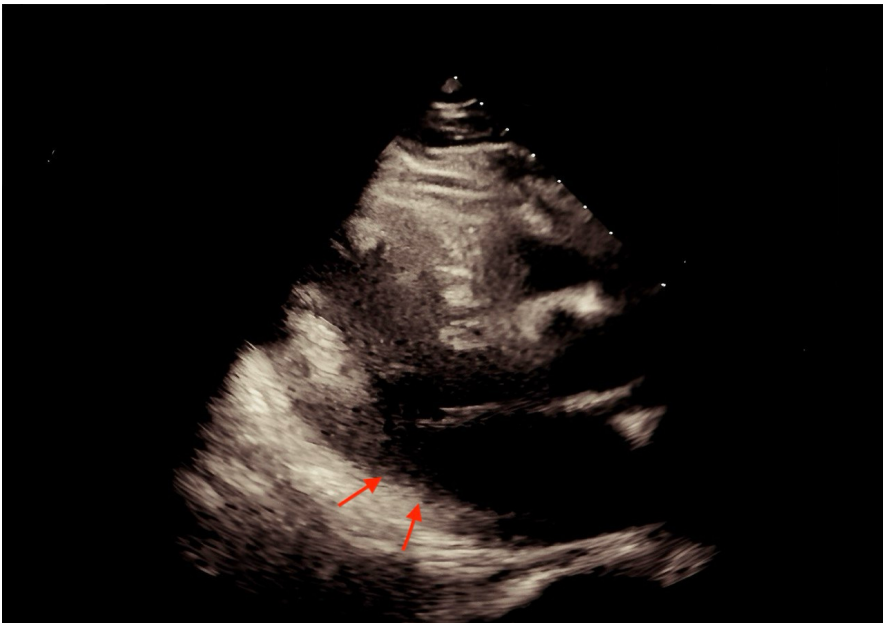
Full TextPDF A 55-year-old woman with a history of type 2 diabetes mellitus, hypertension, smoking, and arteriosclerosis underwent urgent coronary intervention for acute myocardial infarction (AMI). One hour post-procedure, she exhibited deteriorating consciousness, tachypnea, and confusion. Clinical evaluation revealed a hyperosmolar hyperglycemic state (HHS) with metabolic acidosis, which likely contributed to her altered mental status. This case highlights the importance of vigilant monitoring for metabolic complications in patients with diabetes following acute cardiac events. Early recognition and multidisciplinary management are critical to improving outcomes in such scenarios.
Review Article
Abstract
Full TextPDF The study of Piezo channels has significantly advanced our understanding of mechanotransduction in various biological systems, including the cardiovascular system. These channels, particularly Piezo1, have been implicated in a range of physiological and pathological processes, such as heart function, vascular tone regulation, and response to mechanical stress. Despite their crucial role in cardiovascular health, several challenges remain in fully elucidating the mechanisms by which Piezo channels mediate heart function. This review explores the frontiers of Piezo channel research, with a focus on the challenges that hinder progress and potential future directions.
Review Article
Abstract
Full TextPDF Piezo1 channels are mechanosensitive ion channels critical for translating mechanical forces into cellular signals in the cardiovascular system. They regulate heart function by influencing cardiomyocyte contractility and arrhythmogenesis and play a key role in vascular function by modulating endothelial and smooth muscle cell responses to mechanical stimuli. Dysregulation of Piezo1 can contribute to conditions such as arrhythmias, heart failure, and vascular diseases. Despite advancements in understanding Piezo1, challenges remain in studying their mechanisms and developing targeted therapies. Future research into Piezo1’s signaling pathways, the development of selective modulators, and exploring neurovascular interactions hold promise for therapeutic innovations.
Research Article
Abstract
Full TextPDF
Supplementary File Introduction: Unfractionated heparin (UFH) has been the standard anticoagulant for cardiac surgery involving cardiopulmonary bypass (CPB) circuits since 1953. However, there is no universally accepted method for determining the most appropriate dose to achieve the desired activated clotting time (ACT) of at least 480 seconds, or an agreed method for determining the appropriate dose and timing of protamine for heparin reversal.
Methods: A technique for determining an initial heparin dose to achieve a desired ACT was developed for catheter ablation cases in patients with atrial fibrillation. This method also enabled the estimation of an appropriate dose of protamine for reversing the active heparin at the end of the procedure. We evaluated this approach in cardiac bypass cases with additional information being provided by the use of viscoelastic testing.
Results: The method used enabled a single dose of heparin to be found that achieved an ACT of more than 480 seconds in over 82% of cases. A single dose of protamine was effective in reversing the heparin effect after cessation of bypass and patient rewarming in 88.89% of cases.
Conclusion: This study presents a promising, cost-effective approach to managing heparin therapy during coronary bypass (CBP) surgery. Our approach enables an appropriate initial heparin dose to be estimated and determination of a dose of protamine that can be given to adequately reverse active heparin at the end of the procedure, after warming and replacement of pump blood.
Case Report
Abstract
Full TextPDF Rationale: Drug-inducing adverse effects may be critical and fatal. There is a reported serious cardiovascular (CV) presentation with sildenafil. Mitral stenosis (MS) is the most common cause of valvular atrial fibrillation (AF) and flutter. Brugada syndrome (BrS) is a genetic disorder with abnormal electrical activity within the heart that carries a higher risk for ventricular fibrillation and sudden death. Hiatal hernia is a herniation of intra-abdominal contents into the thorax. There is a durable relationship between COVID-19 infection and ischemic heart disease.
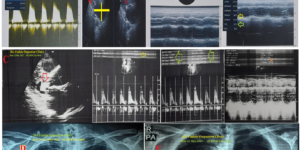
Patient concerns: A 53-year-old, married Egyptian male teacher, mechanically replaced mitral valve (MV) patient was presented to the physician outpatient clinic with intermittent angina within two weeks’ of post-oral sildenafil tablets and COVID-19 pneumonia.
Diagnosis: High lateral ischemia and passed sildenafil-inducing inferior infarction with variable atrial fibro-flutter block, alternative right bundle branch block (RBBB) beat with type II BrS in mechanically replaced MV with recent hiatus hernia and COVID pneumonia.
Interventions: Cardiothoracic surgery, chest X-ray, electrocardiography, echocardiography, and oxygenation.
Outcomes: There is a good outcome despite numerous noteworthy serious risk factors.
Lessons: High lateral ischemia, passed inferior myocardial infarction (MI), variable atrial fibro-flutter block, RBBB beat, BrS, hypocalcemia, recent hiatus hernia, and COVID pneumonia in the mechanically replaced MV are a serious constellation of risk factors. Alternative RBBB beat with type II BrS is newly described. BrS may be transient. Hypocalcemia and Wavy triple ECG sign (Yasser’s sign) are confusing issues for ischemic heart disease.
Research Article
Abstract
Full TextPDF Predisposition to cardiac disease (CD) is currently becoming a common indication for preimplantation genetic testing (PGT). It provides an option for the couplers at risk to avoid the birth of an offspring with a predisposition to CD, as there are no appropriate strategies to prevent CD in the carries of gene mutations predisposing to this condition. The present paper describes the progress in the application of PGT for CD, with its extended application also to carriers of predisposing genes detected through expanded carrier screening (ECS). We present here our experience of 147 PGT cycles for CD, resulting in the birth of 73 children free of predisposing genes to CD, which is a part of our overall PGT series of over one thousand PGT for monogenic disorders (PGT-M). The accumulated experience, presented below, demonstrates considerable progress in using PGT to avoid the birth of children with a genetic predisposition to CD.
Research ArticleWithers K*, Raby K, Parker W, German C, Eyadiel L, Hilton T, Goslen K, Green S, Banoian D, Bapat S, Thomas A, Seals A4 and Pisani B
Continuation of Beta Blockers in Patients on Inotrope Therapy: A Counterintuitive Dilemma Read More »
Introduction: Cardiogenic shock (CS) and acute decompensated heart failure (ADHF) are states of low cardiac output that manifest as tissue hypoperfusion and end-organ damage. Current guidelines do not provide recommendations regarding beta blocker (BB) use in CS. This study sought to analyze the effects of BB continuation on in-hospital mortality among patients admitted with ADHF necessitating inotropic therapy.
Methods: A single-center, retrospective study was conducted in adult patients hospitalized with ADHF requiring inotropes over a three-year period. Patients with CS were stratified based on the Society for Cardiovascular Angiography and Interventions (SCAI) classification of CS and Get With The Guidelines-Heart Failure (GWTG-HF) risk score. BB continuation was assessed at admission and was defined as administration for at least 50% of the hospital stay. A time-to-event analysis framework was implemented using Cox proportional hazards models to analyze the effect of BB continuation on in-hospital mortality.
Results: A total of 449 patients were included in the study. Twelve patients were excluded, as there was insufficient data to calculate the GWTG-HF risk score. A significant mortality benefit was seen with BB continuation in all statistical models. When adjusted for SCAI and GWTG-HF risk score, BB continuation was associated with a 65% reduction in in-hospital mortality [HR 0.35 95% CI 0.19-0.64, p = 0.0008].
Conclusion: In select patients with ADHF resulting in CS, there appears to be a mortality benefit associated with continuation of BB on admission that remains significant after adjustment for severity of CS.
Research Article
Abstract
Full TextPDF Recent advances in biomedical applications have focused a lot of emphasis on the detection of what could be caused by cardiovascular disease (CVD). The electrocardiogram (ECG), which depicts the electrical activity of the heart, is the foundation for arrhythmia analysis. Different machine learning methods used on ECG datasets have demonstrated excellent performance in detecting arrhythmias. Nevertheless, feature extraction is necessary for machine learning algorithms. Modern deep learning techniques don't require feature extraction because they learn all the parameters simultaneously, in contrast to these techniques. In this study, a 1D convolutional neural network (CNN) approach is presented and tested on the arrhythmia database of the Massachusetts Institute of Technology-Beth Israel Hospital (MIT-BIH). The proposed model, which only has three layers, attained an accuracy of 97.40%.
Case Report
Abstract
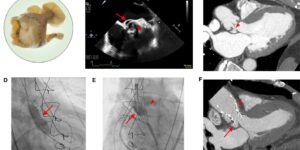
Full TextPDF An 84-year-old man with a Shelhigh Super Stentless valve presented for valve-in-valve (ViV) transcatheter aortic valve replacement (TAVR). Given the lack of radiopaque markers and the presence of a non-coronary cusp (NCC) pseudoaneurysm, implant depth was guided by root aortography at the time of balloon aortic valvuloplasty (BAV) using a pigtail in the right coronary cusp (RCC).
Case Report
Abstract
Full TextPDF Incessant ectopic atrial tachycardia (EAT) is well-known in the electrophysiology world. However, once accompanied by neurological manifestations, hence is a dilemma. We are reporting a 26-year-old male presenting with incessant symptomatic EAT. Once cardioverted, he began to manifest cardiovascular stroke clinical symptoms. Further objective investigation revealed no evidence of cardioembolic stroke. Our aim of this case report is to explore if there is a true correlation between EAT and possible neurological association and open further guidelines related to research.