Abstract
Introduction: Congestive heart failure (CHF) accounts for significant medical costs and patient mortality. There are ways to mitigate these parameters by providing patient and provider education, optimizing medications, and applying life-saving devices with a referral for a left ventricular assist device (LVAD) when appropriate. We retrospectively observed the charts of 40 patients at our Dayton Veterans Affairs Medical Center (VAMC) for areas of improvement.
Methods: Charts were manually reviewed over 2019 for ejection fraction (EF) at the time of diagnosis and ischemic cardiomyopathy (ICM) vs. nonischemic cardiomyopathy (NICM) etiology of heart failure. Information on the titration of beta-blockers (BB), angiotensin-converting enzyme inhibitors (ACE-I), angiotensin receptor blockers (ARBs), and advanced heart failure medications was collected. Readmission rates and heart failure follow-up appointment rates were gathered, and further details were investigated regarding the application of a life vest and automatic implantable cardioverter-defibrillator (AICD) when clinically appropriate.
Results: Median EF for patients was 34%, consistent with systolic heart failure. 65% of patients had ICM. For medications, BB was maximally titrated for 85% of patients within a wide data range. ACE-I/ARBs titration was appropriate in 75% of patients. An average of 4.7 dose adjustments for BB and 3.6 dose adjustments for ACE-I/ARBs occurred. Advanced CHF medications were rarely prescribed. Exacerbation rates were 60%, from 1–5 readmissions and an average of 1.07 readmissions. 98% of patients received CHF-specific follow-up after each CHF admission. 60% were eligible for advanced life support devices, 25% were offered life vests, and 62% were offered AICD. No patient was referred to a tertiary center for LVAD.
Conclusion: We should work towards 100% medication titration to improve outcomes, especially BB which is known to have morbidity value. We can continue to reduce heart failure readmission rates by providing patient and provider education and continuing to do well at heart failure follow-up appointments. Life vest and AICD should be offered more consistently, and tertiary referral to receive LVAD should remain offered per standard of care.
Keywords
congestive heart failure, advanced heart failure, readmission, Veterans Affairs, life-saving device, life vest, left ventricular assist device, automatic implantable cardioverter-defibrillator, angiotensin receptor-neprilysin inhibitor, beta-blockers
Abbreviations
CHF: congestive heart failure; LVAD: left ventricular assist device; VAMC: Veterans Affairs Medical Center; EF: ejection fraction; ICM: ischemic cardiomyopathy; NICM: nonischemic cardiomyopathy; BB: beta-blockers; ACE-I: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; AICD: automatic implantable cardioverter-defibrillator; CMS: Centers for Medicare and Medicaid Services; BNP: brain natriuretic peptide
Introduction
The Centers for Disease Control (CDC) establishes that heart failure is responsible for high medical costs and carries an associated mortality risk with it [1]. About half of people with heart failure die within 5 years of diagnosis, and the yearly estimated cost is 30.7 billion USD [2–4]. It is therefore important for patient morbidity and mortality as well as resource utilization to manage heart failure in a guideline-directed stepwise fashion [5] and to work towards decreased readmission rates as a measure of stable disease.
We wished to assess how our facility at the Veterans Affairs Medical Center (VAMC) compared nationally for this comorbid illness by the measure of medication titration to a goal of patient maximally tolerated dose and how much time this took as well as the addition of advanced heart failure medications, congestive heart failure (CHF) readmission rates, CHF follow-up appointments following discharge, if life vest or automatic implantable cardioverter-defibrillator (AICD) were placed when appropriate, and referral to a tertiary center for left ventricular assist device (LVAD) as not provided at this VAMC.
Methods
Charts were manually reviewed over the year 2019 and the data was retrospectively observed for 40 patients, all of whom were male and the majority White race. Information was collected for ejection fraction (EF) at the time of diagnosis, etiology of heart failure, and if ischemic cardiomyopathy (ICM) or nonischemic cardiomyopathy (NICM) was present as diagnosed on left heart catheterization (LHC). Medication doses were evaluated for titration of beta-blockers (BB), angiotensin-converting enzyme inhibitors (ACE-I), or angiotensin receptor blockers (ARBs), and if advanced heart failure medications were added such as ivabradine, a sodium funny channel inhibitor. We observed heart failure readmission rates for the sample patients and looked for follow-up appointments to observe if these were completed to the system standard. Further, we looked at life vest and AICD placement rates when appropriate and if the patients had been referred to a tertiary care center for LVAD placement.
All the data was collected and calculated manually, given the paucity of other sorting systems within the VAMC electronic medical record (EMR): The Veterans Health Information Systems and Technology Architecture (VISTA).
Results
The Centers for Medicare and Medicaid Services (CMS) released a report in 2017 with trends for hospital readmissions for acute myocardial infarction (AMI), chronic obstructive pulmonary disease (COPD), CHF, pneumonia, and stroke [5]. Trends for heart failure readmission rates across 2820 hospitals were 21.6% from July 2013–June 2014, 21.8% from July 2014–June 2015, and 21.4% from July 2015–June 2016. The Dayton VAMC uses Report Central Veterans Integrated Services Networks (VISN), which only notes trends from October 2015 to 2019 [6]. From this data, our facility comparison to national readmission rates for heart failure is similar to or better than the national average, with data as follows (Table 1).
While the data shows that our facility performs better than VAMC nationally on the quality measure of heart failure readmissions, other intrinsic parameters also needed to be investigated. These included medication titration to goal, the addition of advanced heart failure medications, and CHF follow-up appointments. Additionally, if a life vest or AICD were placed when appropriate and referral to a tertiary center for LVAD, as the procedure and device were not provided at this VAMC.
| Nationally, VAMC (2820 hospitals) | Dayton VAMC |
| July 2013–June 2014 21.6% | Not in VISN |
| July 2014–June 2015 21.8% | Not in VISN |
| July 2015–June 2016 21.4% | Oct 2015–Sept 2016 19.7% |
| Not released by CMS | Oct 2016–Sept 2017 22.7% |
| Not released by CMS | Oct 2017–Sept 2018 11.5% |
| Not released by CMS | Oct 2018–Sept 2019 17.7% |
Table 1: CMS and VISN comparators for heart failure readmission rates.
We found that ICM was present in 65% (26/40) of patients, and the most common etiologies were atherosclerotic, followed by hypertensive disease and dilated cardiomyopathy. Other less common causes included cocaine abuse, post-radiation therapy with or without chemotherapy, and significant alcohol abuse, in that order. EF at diagnosis ranged from < 15–55% and the median EF was 34%.
For BB titration, 85% (32/40) of patients had titration to goal. Two patients were at a target dose of their BB before the diagnosis of heart failure and it took a wide range, 1 day to 13 years, for patients to reach the target dose if achieved. For ACE-I or ARBs, there were 75% (30/40) of patients in which titration occurred. Five patients were at a target dose of their ACE-I or ARBs before the diagnosis of heart failure and it took 5 days to 8 years for patients to reach the target tolerated dose. For patients where titration occurred, an average of 4.7 dose adjustments of BB were performed and 3.6 dose adjustments of ACE-I or ARBs were performed to tolerated blood pressure. Only one patient (2.5%) of our study set was prescribed an angiotensin receptor-neprilysin inhibitor (ARNI). No patient had been started on ivabradine (Figure 1).
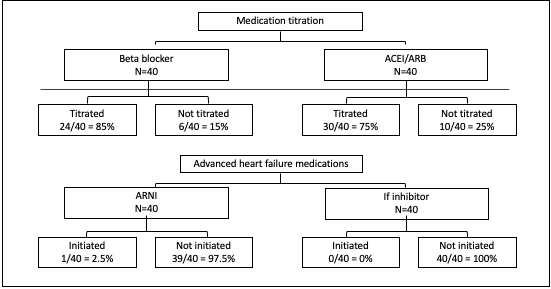 Figure 1: Medication titration to maximally tolerated dose.
Figure 1: Medication titration to maximally tolerated dose.
Heart failure exacerbation rates were clinically noted in 60% (24/40) of patients, ranging from 1–5 readmissions with an average of 1.07 readmissions per patient. Nearly all patients received a referral for heart failure follow-up with each admission. Appointments were canceled when a patient refused to come to the facility for care because he or she was “too tired,” for example, or “already had an appointment” with the outpatient general cardiology clinic. Some patients who would not come to the clinic for follow-up would later be provided home health services. Patients did seem to have reliable transportation, and the concern was addressed in all cases reviewed.
Regarding advanced heart failure life-saving devices, 60% (24/40) of patients were eligible candidates for life vest and AICD. 25% (6/24) were offered a life vest during the duration of treatment for heart failure, however, only 4 accepted and 2 declined. From this number, 2/4 that had life vest placement had gone on to receive AICD. For those two patients, it took 4–6 months to receive AICD, including the 3 months necessary follow-up for persistently low EF. The other two patients with life vests had marked enough improvement in their EF that they no longer required AICD placement. 62% (15/24) of the sample patients were offered AICD. Two declined so 86% (13/15) of those offered successfully received an AICD. No patient had been referred to a tertiary center for LVAD (Figure 2).
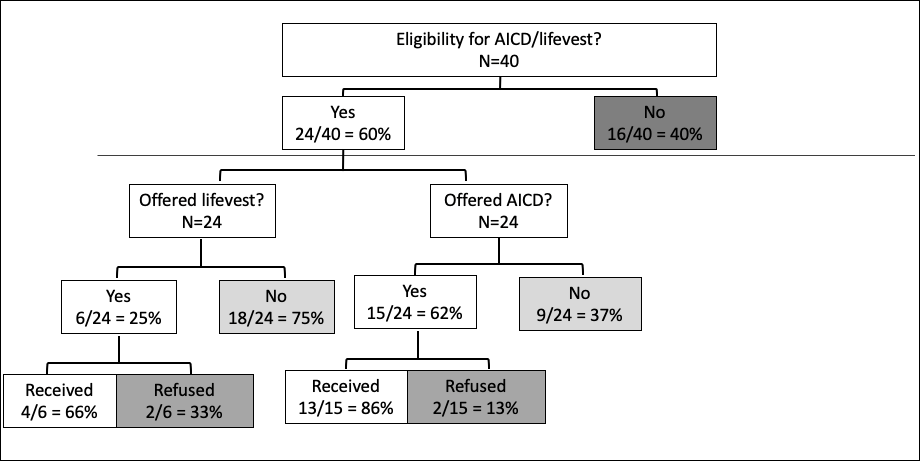 Figure 2: Eligibility distributions of AICD and life vest.
Figure 2: Eligibility distributions of AICD and life vest.
Discussion
We were able to identify objective data about medications. Appropriate up-titration of medications occurred for BB 85% of the time and for ACE-I or ARBs 75% of the time. In some patients, up-titration occurred as quickly as one day to the tolerated dose but for some patients, medications were up-titrated to optimal therapy over years. This may be reflected in parts by multiple factors including patient physiology and their respective comorbidities that allow for medication tolerance such as coexisting kidney disease, lung disease, coronary disease, pulmonary hypertension, and intrinsic blood pressure response. Readmissions seemed to increase with how often heart failure medications were adjusted. When dose adjustments occurred, BB were adjusted an average of 4.7 times and ACE-I or ARBs were adjusted an average of 3.6 times. This may be related to the feature of BB that they affect heart rates as well as neurohormonal remodeling of the heart in heart failure which is responsible for its greater mortality benefit. BB are the most important to titrate [7].
While the newer advanced heart failure medications are recommended, only one patient was started on sacubitril/valsartan, the prototypical ARNI, and no patients were started on ivabradine. This could have been due to poor understanding by providers about when to start the medication, when to refer to cardiology when the patient is a candidate for these therapies, a specialist missing the opportunity to start the medication, or a patient’s failure to follow up at subsequent cardiology appointments when the medication would have been started. These are separate multifactorial details from the perspective of patient education, provider education, and patient autonomy. Regarding information to the provider, patients should now be switched to sacubitril/valsartan when New York Heart Association (NYHA) class II or III systolic heart failure is present and they have tolerated an ACE-I/ARB after a 36-h washout period. This is a level I recommendation by the American College of Cardiology Heart Failure Guideline 2017 [5]. It is important to understand and therefore expound on these advanced heart failure medications further.
ARNIs work by two mechanisms, one is that of an angiotensin receptor blocker, which blocks angiotensin II from binding muscles around blood vessels and causing vasoconstriction, and the second is the component sacubitril, which inhibits the enzyme neprilysin. Neprilysin is responsible for the conversion of several compounds, namely bradykinin and angiotensin II to the natriuretic peptides. Brain natriuretic peptide (BNP) is the clinically measured natriuretic peptide. Under physiologic conditions, bound BNP receptors activate guanylyl cyclase and catalyze cyclic guanosine monophosphate (cGMP) which affects protein kinase G to vasoconstrict and decreases blood pressure, sympathetic tone, and aldosterone levels, and causes diuresis. ARNIs should be started after the ACE-I has been discontinued for 36 h and should not be given if a patient has a history of angioedema [8].
Ivabradine is another agent that can be started for symptomatic treatment of stable angina and heart failure not completely managed by a maximum dose of BB or with contraindications to BB. Candidacy for initiation is addressed in the 2010 Systolic Heart Failure Treatment with the If Inhibitor Ivabradine Trial (SHIFT). Indications are symptomatic heart failure, reduced EF < 35%, sinus rhythm > 70 bpm, admission for heart failure within the previous year, and stability on background treatment, including BB if tolerated. It should be started at a dose of 5 mg twice a day with food for 14 days, followed by titration to a maximum of 7.5 mg twice a day as tolerated. The goal resting heart rate on this medication is 50–60 bpm with heart rate reduction by about 10 bpm at the site of the cardiac funny channel in the sinoatrial node. It is the first hyperpolarization-activated cyclic nucleotide-gated (HCN) channel blocker and does not affect blood pressure, intracardiac conduction, myocardial contractility, or ventricular repolarization. An important side effect of ivabradine is that it may decrease sensitization to bright lights via the retinal current [9].
Heart failure exacerbation rates seemed to remain high at 60% (N = 24) in our sample of 40. However, per VISN, the facility was at 17.7% admissions for overall medical conditions given primary diagnosis coded in the admission charge. Readmissions averaged 1.07 per patient, ranging from 1–5 readmissions per patient for the VAMC. Of note, a limitation was if an individual presented to an alternate hospital system, it was unable to be recorded as a visit due to a lack of tracking ability. A competitor hospital in the Southwest Ohio region has 13 hospital sites and a second hospital system has 5. This is a higher number of facilities per patient per capita nationwide.
Nearly, all patients received a referral for heart failure follow-up with each admission, a reflection that our site does well for this standard. Appointments were canceled when a patient refused to come to the facility for care because he or she was “too tired,” for example, or “already had an appointment” with the outpatient general cardiology clinic and felt that another appointment was redundant. Some patients who would not come to the clinic for follow-up would later be provided home health services. Patients did seem to have reliable transportation, and the concern was addressed in all cases reviewed.
Regarding advanced heart failure life-saving devices, more than half of patients were eligible candidates for life vests and AICD, while sub-optimally 17% (4/24) went on to receive a life vest. Two further patients were recommended a life vest but declined. AICD was offered to 62% percent (15/24) of patients, 54% (13/24) received it and two declined. From this number, 2/4 that had life vest placement went on to receive AICD. For these two patients, it took 4–6 months to receive AICD, including the 3 months necessary follow-up for persistently low EF guidelines. The other two patients with life vests had marked improvement in their EF so they no longer required AICD placement. For 9 patients who bypassed AICD, without a prior life vest, it took between 2 months to 12 years for placement. No patient had been referred to a tertiary center for LVAD.
It is unclear why patients had not been referred to a tertiary center for care, but all patients had one or more significant comorbidities including chronic or end-stage renal disease, substance abuse concerns, cancers, concomitant respiratory disease, further myocardial infarctions and cardiac procedures, and infections. It is possible that management of these other underlying issues provided more immediate benefit to the patient while they were receiving care than that of a heart resuscitative device. Of the patients who had died, there were 13, one was noted to die of heart failure as the primary cause and had transitioned to hospice services. He was among two refusing AICD placement.
Conclusion
In summary, we can work to improve numbers for medication up-titration to 100% of patients with careful documentation when this cannot be done for patient autonomy or tolerance of dose due to issues like hypotension and syncope. We can continue to work on the reduction of heart failure readmission rates by providing patient and provider education and continuing to do well at heart failure follow-up appointments. There are a variety of reasons for the sub-optimal numbers related to a life vest and AICD placement, these patients, fortunately, did not die in the meantime, and this is a measure we note on which to improve. LVAD is an invasive device and a significant surgery so patients should be well-educated. It may be helpful to have a specialized staff member share this particular device, surgery, and indication at routine follow-up appointments when patients meet criteria, before any referral. Patients may not want the procedure or are not surgical candidates, however, we did not find a further conversation in this regard in the chart notation.
Funding
This research did not receive grant funding from agencies in the public, commercial, or not-for-profit sectors.
Credit Authorship Contribution Statement
The primary and sole author contributed to the data collection, creation of figures and tables, manuscript writing, and editing.
Declaration of Competing Interest
The author declares no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Information for Laboratories about Coronavirus (COVID-19).
- Bytyçi I, Bajraktari G. Mortality in Heart Failure Patients. Anatol J Cardiol. 2015;15(1):63-68.
- Henkel DM, Redfield MM, Weston SA, et al. Death in Heart Failure: A Community Perspective. Circ Heart Fail. 2008;1(2):91-97.
- Patel J. Heart Failure Population Health Considerations. Am J Manag Care. 2021;27(9 Suppl):S191-S195.
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
- CMS. Veterans Health Administration Hospital Performance Data.
- Chavey WE 2nd. The importance of beta blockers in the treatment of heart failure. Am Fam Physician. 2000 Dec 1;62(11):2453-462.
- Menendez JT. The Mechanism of Action of LCZ696. Card Fail Rev. 2016;2(1):40-46.
- Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 2010;376(9744):875-85.
