Stein EJ1, Elison D 1, Cham MD2, Aldea G3, McCabe JM1 and Chung CJ*1
1, Cham MD2, Aldea G3, McCabe JM1 and Chung CJ*1
1Division of Cardiology, Department of Medicine, University of Washington Medical Center, Seattle, WA, USA
2Department of Radiology, University of Washington Medical Center, Seattle, WA, USA
3Division of Cardiothoracic Surgery, Department of Surgery, University of Washington Medical Center, Seattle, WA, USA
*Correspondence: Christine J. Chung, Division of Cardiology, Department of Medicine, University of Washington Medical Center, Seattle, WA, USA
Received on 12 November 2023; Accepted on 23 January 2024; Published on 25 January 2024
Copyright © 2024 Stein EJ, et al. This is an open-access article and is distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
An 84-year-old man with a Shelhigh Super Stentless valve presented for valve-in-valve (ViV) transcatheter aortic valve replacement (TAVR). Given the lack of radiopaque markers and the presence of a non-coronary cusp (NCC) pseudoaneurysm, implant depth was guided by root aortography at the time of balloon aortic valvuloplasty (BAV) using a pigtail in the right coronary cusp (RCC).
Keywords
TAVR, valve-in-valve, balloon aortic valvuloplasty, Shelhigh, stentless
Abbreviations
TAVR: transcatheter aortic valve replacement; TEE: Transesophageal echocardiography; LV: left ventricle; ViV: valve-in-valve; NCC: non-coronary cusp; CTA: computed tomographic angiography; TEE: transesophageal echocardiogram; BAV: balloon aortic valvuloplasty; TTE: transthoracic echocardiography; RCC: right coronary cusp; LVOT: left ventricular outflow tract
Learning Objectives
- Understand how a sinus of Valsalva aneurysm and a sutureless surgical aortic valve can disrupt conventional landmarking technique during a transcatheter aortic valve replacement (TAVR).
- Discuss alternative TAVR guidance strategies in the case of disrupted anatomy.
Case Presentation
An 84-year-old man with a history of surgical aortic valve replacement in 2005 with a 25 mm Shelhigh™ (Union, NJ) Super Stentless porcine valve (Figure 1A) presented with acutely decompensated heart failure. The Shelhigh valve is a stentless porcine valve contained within a radiolucent sewing ring with three commissural posts [1]. The valves were discontinued due to issues with sterility and early degeneration. Transesophageal echocardiography (TEE) revealed prosthetic valve degeneration resulting in severe aortic regurgitation (Supplemental Video 1 and 2) and a globally hypokinetic left ventricle (LV) with ejection fraction of 25–30%. He was referred for valve-in-valve (ViV) TAVR.
A sinus of Valsalva pseudoaneurysm involving the non-coronary cusp (NCC) was identified on TEE. Cardiac computed tomographic angiography (CTA) demonstrated extension inferiorly into the LV outflow tract (Figure 1B and 1C). Given the patient’s advanced age and prior sternotomy, he was not a surgical candidate, and we proceeded with ViV TAVR via transfemoral access.
The internal diameter of the Shelhigh valve measured 19 mm on cardiac CTA, so we planned to implant a 23 mm Medtronic Evolut FX valve (Minneapolis, MN) to allow for adequate oversizing. A balloon aortic valvuloplasty (BAV) with an 18 mm True balloon was performed with simultaneous aortic root angiography to confirm appropriate prosthesis sizing and demonstrate the location of the constrained portion of the valve at which anchoring would occur (Figure 1D). Since the NCC could not be used to guide implant depth, the coplanar view with the pigtail catheter in the right coronary cusp (RCC) (Figure 1E) was utilized instead (Supplemental Video 3).
Finally, the 23 mm Evolut FX valve was advanced across the aortic valve and deployed during rapid ventricular pacing at 140 beats per minute (Supplemental Video 4). Given the small size of the surgical prosthesis, there was “watermelon-seeding” of the Evolut FX valve into the aorta, but after several deployment attempts, the desired implant depth of 3–5 mm was achieved. Postoperative transthoracic echocardiography (TTE) showed no perivalvular leak (Supplemental Video 5). Repeat CTA at 30 days demonstrated the Evolut valve at the desired depth of implant (Figure 1F).
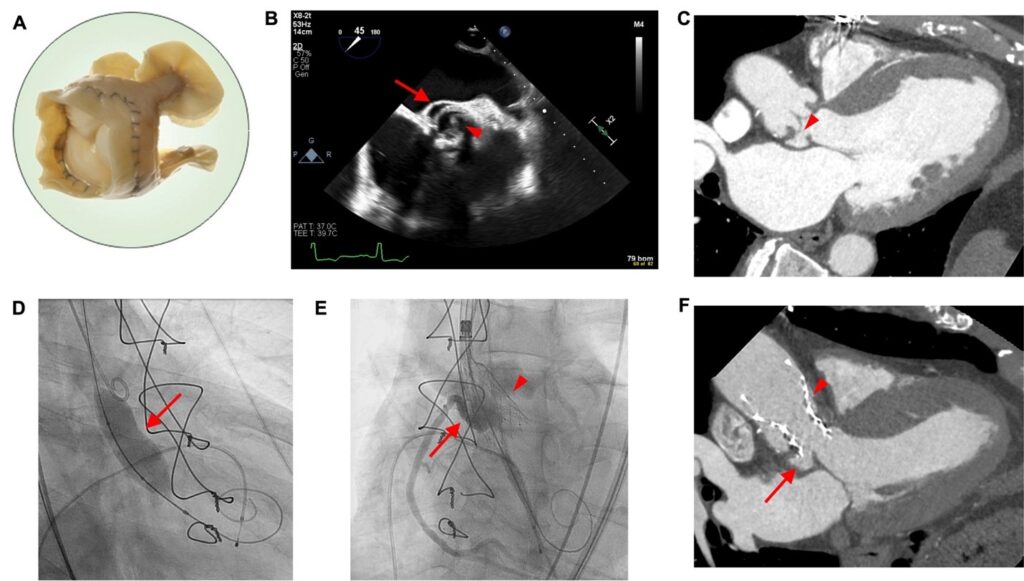 Figure 1: (A) Photograph of the Shelhigh valve, (B) transesophageal echocardiographic short axis view of the Shelhigh valve (arrowhead) and non-coronary cusp (NCC) aneurysm (arrow), (C) computed tomographic angiography (CTA) 3-chamber view of the Shelhigh valve and non-coronary cusp aneurysm (arrowhead), (D) balloon aortic valvuloplasty during TAVR with arrow denoting the waist on the balloon, (E) partial deployment of Evolut TAVR valve (arrowhead) during aortography showing the right coronary cusp as a fiducial depth marker (arrow), and (F) 30-day follow up CTA showing final position of the TAVR (arrowhead) spanning the NCC aneurysm (arrow). (A) reproduced from Cattaneo et al. [1].
Figure 1: (A) Photograph of the Shelhigh valve, (B) transesophageal echocardiographic short axis view of the Shelhigh valve (arrowhead) and non-coronary cusp (NCC) aneurysm (arrow), (C) computed tomographic angiography (CTA) 3-chamber view of the Shelhigh valve and non-coronary cusp aneurysm (arrowhead), (D) balloon aortic valvuloplasty during TAVR with arrow denoting the waist on the balloon, (E) partial deployment of Evolut TAVR valve (arrowhead) during aortography showing the right coronary cusp as a fiducial depth marker (arrow), and (F) 30-day follow up CTA showing final position of the TAVR (arrowhead) spanning the NCC aneurysm (arrow). (A) reproduced from Cattaneo et al. [1].
Discussion
ViV TAVR is more challenging in stentless valves without fluoroscopically visible markers. Adjustment of fluoroscopic angles to minimize parallax in the radio-opaque posts of a stented valve reduces left ventricular outflow tract (LVOT) and implant foreshortening, improving the accuracy of deployment depth. In the absence of fluoroscopic landmarks, the constrained portion of the Shelhigh valve, corresponding to the sewing ring, was identified using a non-compliant balloon (Figure 1D), which, when inflated with simultaneous aortography, also confirmed the internal diameter obtained on CTA used for sizing of the transcatheter prosthesis.
Conclusion
This represents the first published report of a successful ViV TAVR in the Shelhigh stentless porcine valve. The case demonstrates the role of cardiac CTA in preprocedural planning and sizing of the internal diameter of an uncommon surgical bioprosthesis, which was significantly smaller than its labeled external diameter. It also highlights the use of BAV to demonstrate the constrained waist of a radiolucent bioprosthesis and the adequacy of using the coplanar view and RCC to guide implant depth in the presence of distorted NCC anatomy.
Consent
Written informed consent was obtained from the patient prior to performing all procedures described herein. Verbal consent was obtained from the patient for the research, writing, and publication of this article.
Conflicts of Interest
James M. McCabe consults for Edwards Lifesciences, Medtronic, and Boston Scientific and holds equity in ConKay Medical and Excision Medical. Christine J. Chung reports consulting fees/honoraria from Boston Scientific, Edwards Lifesciences, and Medtronic. The remainder of the authors have nothing to disclose.
Funding
No sources of funding were used for the present case report.
Supplementary Material
The supplementary material for this article can be found online at:
Supplemental Video 1: Transesophageal echocardiogram short-axis view of the Shelhigh valve and non-coronary cusp aneurysm.
Supplemental Video 2: Transesophageal echocardiogram long axis view of the degenerated Shelhigh valve and severe aortic regurgitation.
Supplemental Video 3: Intraoperative fluoroscopy exhibiting the balloon aortic valvuloplasty.
Supplemental Video 4: Intraoperative aortography at the right coronary cusp during partial deployment of the transcatheter aortic valve.
Supplemental Video 5: Intraoperative post-deployment transesophageal echocardiography demonstrating the final position of the transcatheter aortic valve replacement without perivalvular leak or aortic regurgitation.
References
