asystole, pacemaker, lead fracture, cardiac arrest, electrophysiology
ED: emergency department; AICD: automatic implantable cardioverter-defibrillator; AV: atrioventricular; ECG: electrocardiogram; LV: left ventricular; RV: right ventricular; TVP: temporary transvenous pacing; CRT-D: cardiac resynchronization therapy-defibrillator
A pacemaker is a small device implanted in the chest to help control the heartbeat. A pacemaker lead is a thin, flexible wire inserted into a vein and passed through to the heart, where it delivers electrical impulses to the heart muscle to maintain a proper heartbeat. Lead fracture is a rare but serious complication that can occur in patients with pacemakers [1].
Symptoms of a lead fracture include chest pain, shortness of breath, and loss of pulse. In some cases, the fracture can cause the lead to move into an abnormal position, which can damage the heart or lungs. If the lead is not removed, it can cause serious complications such as infection, bleeding, or even death.
The causes of lead fracture can include normal wear and tear on the lead over time, as well as trauma to the chest or heart. Additionally, certain pacemaker models and manufacturers have been associated with higher rates of lead fracture. When a pacemaker lead fractures, it can become disconnected from the electrode and stop transmitting electrical signals to the heart [2]. This can cause the heart to stop beating, leading to a life-threatening condition called asystole.
A 72-year-old Caucasian male presented to the emergency department (ED) with multiple automatic implantable cardioverter-defibrillator (AICD) shocks while lying in bed at home with a history of non-ischemic cardiomyopathy, congestive heart failure, complete atrioventricular (AV) block with a defibrillator, and atrial flutter. The patient states he felt lightheaded prior to the defibrillator firing, which he continued to experience en route to the hospital by Emergency Medical Services (EMS). On arrival at the ED, the patient had visual AICD firing at which time the patient was placed on cardiac telemetry, and a Medtronic rep was contacted for interrogation of the device. His vitals were as follows: blood pressure 130/59, pulse of 78, temperature 98.2°F, respiratory rate of 17, and SpO2 of 92%. Physical exam was mostly benign other than AICD palpable in the left upper chest. Labs showed sodium 140 mmol/L, potassium 4.3 mmol/L, chloride 105 mmol/L, CO2 24 mmol/L, anion gap 11, blood urea nitrogen 25 mg/dL, creatinine 1.64 mg/dL, calcium 9.5 mg/dL, magnesium 2.2 mg/dL. High sensitivity troponins were elevated at 798 ng/L, and ECG showed a ventricular-paced rhythm with a rate of 78 as shown below (Figure 1).
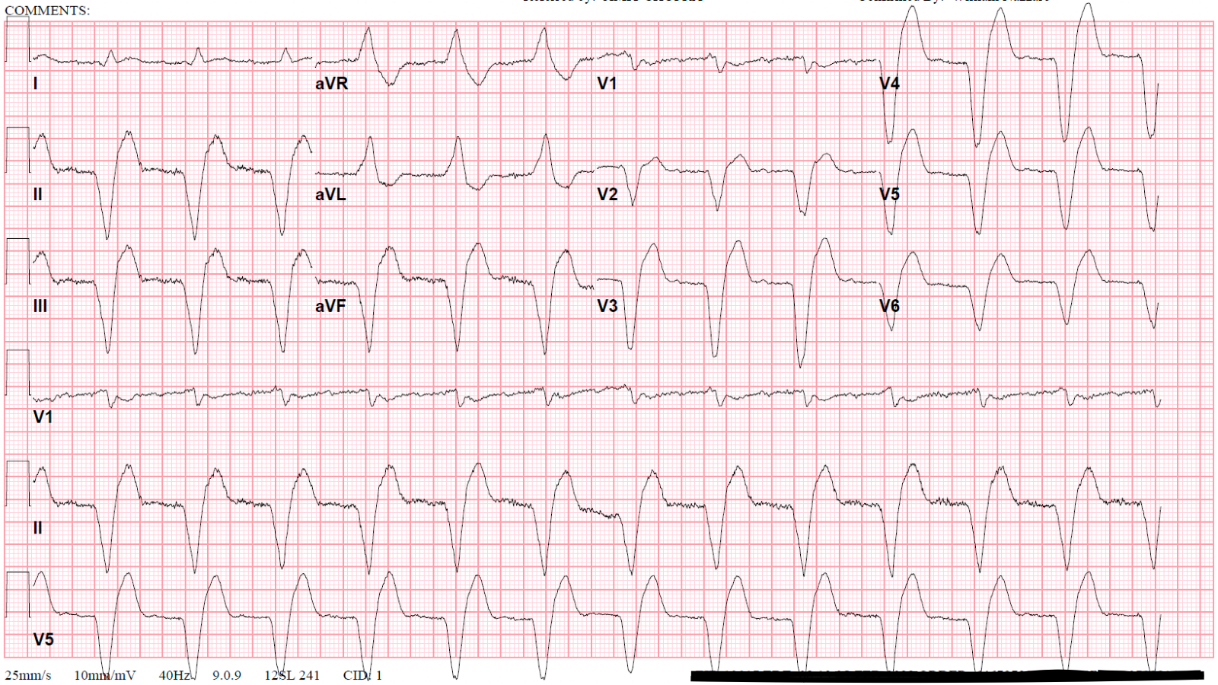
Figure 1: The ECG showing a ventricular-paced rhythm.
While at the hospital, the patient would become asystolic each time he raised his arm. As the patient became unresponsive, his arm would fall back to a neutral position, at which point he would regain consciousness and resume his conversation from prior to the asystole episode. Pacemaker interrogation revealed that the patient had a total of 6 asystolic episodes throughout the day, one of which was captured on the following rhythm strip (Figure 2).
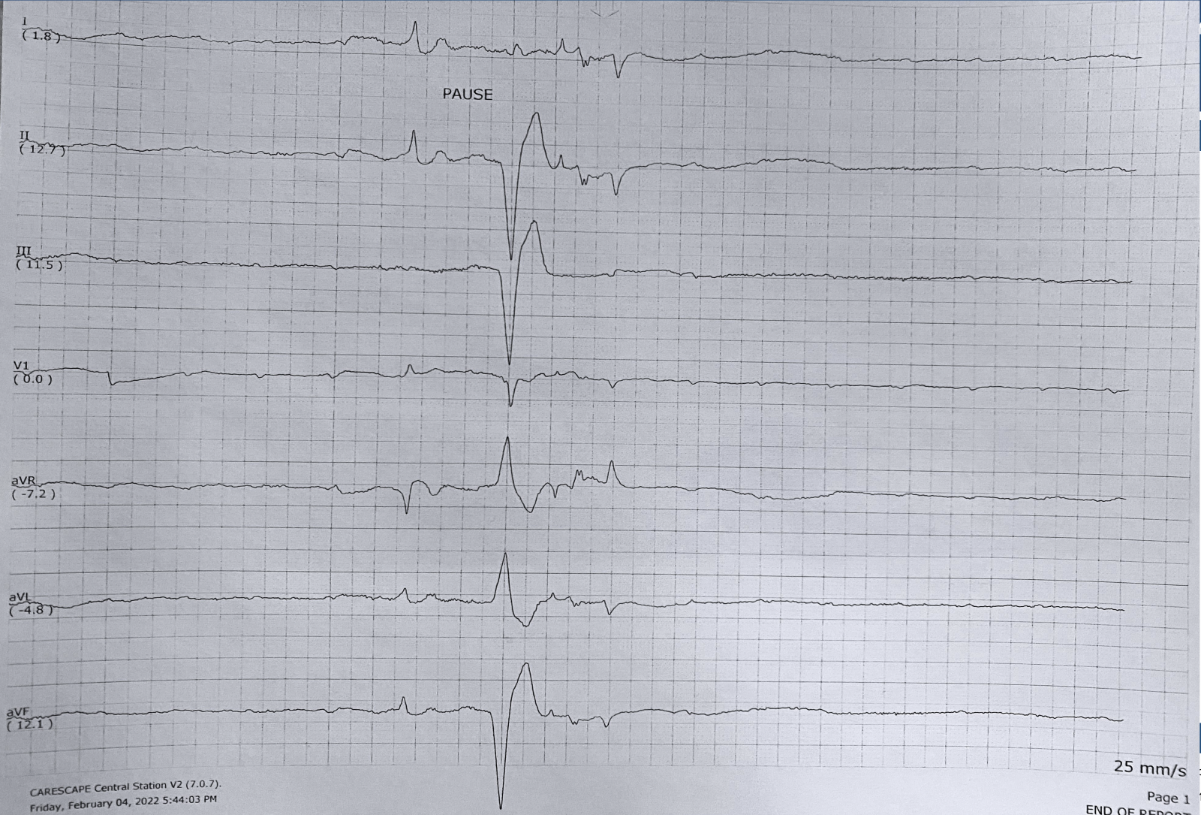
Figure 2: Asystolic episode captured on the rhythm strip.
Chest X-ray showed left ventricular (LV) lead failure and right ventricular (RV) lead fracture, leading to AV blocks and pacing inhibition. It was determined that the arm movement would disconnect the leads, leading to asystole, as the patient was completely dependent on the pacer. A temporary transvenous pacing (TVP) was placed in the ED with a rate of 80, and the pacemaker was set with a backup rate of 50 as per the cardiology recommendation. The patient was admitted to the ICU, and seen by an EP cardiologist, underwent a successful upgrade of his AICD to biventricular pacer, and the TVP was removed.
Chest X-ray showing patient left AICD and right IJ approach TVP placed shown below (Figure 3).
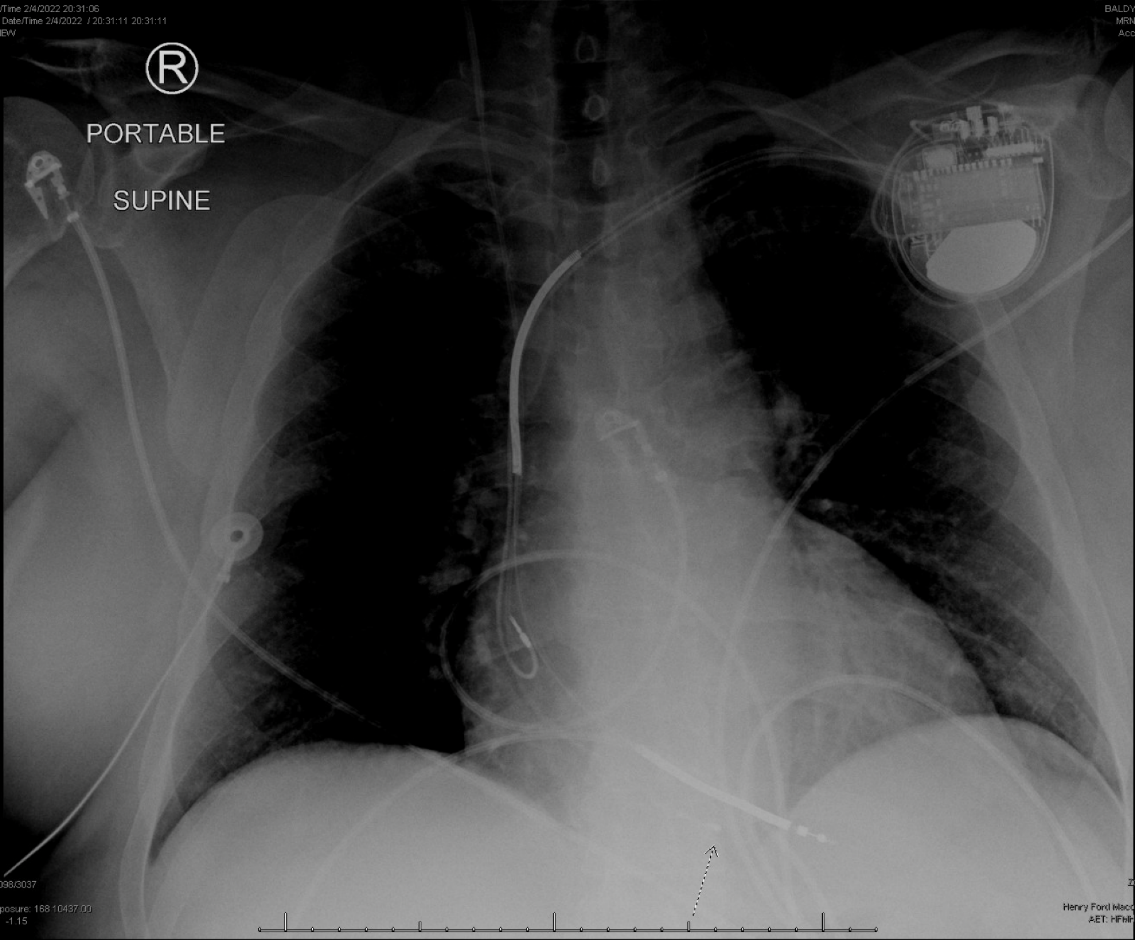 Figure 3: Chest X-ray showing patient’s left AICD and right IJ approach TVP placed.
Figure 3: Chest X-ray showing patient’s left AICD and right IJ approach TVP placed.
Chest X-ray after device upgrade from ICD to cardiac resynchronization therapy-defibrillator (CRT-D) with new RV and LV lead placement is shown below (Figure 4).
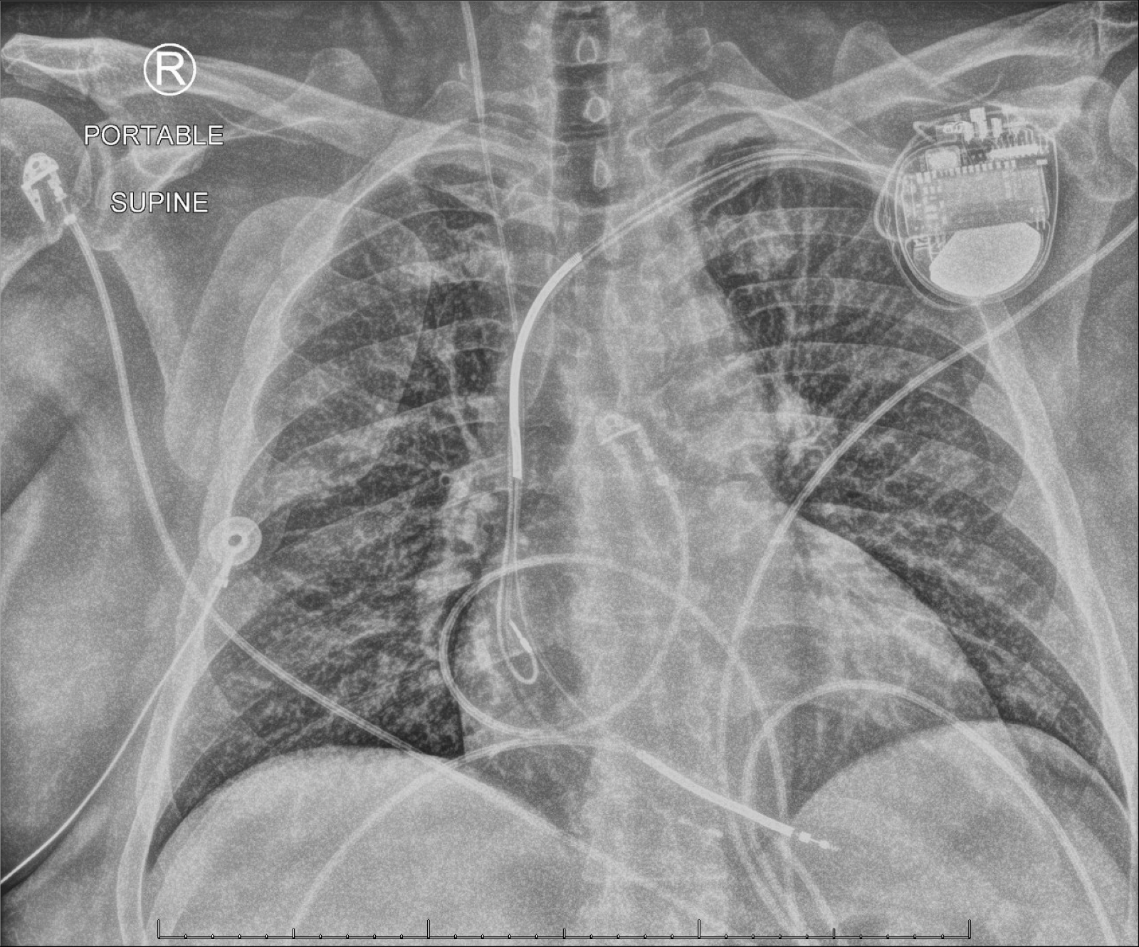 Figure 4: Chest X-ray after device upgrade from ICD to cardiac resynchronization therapy-defibrillator (CRT-D) with new RV and LV lead placement.
Figure 4: Chest X-ray after device upgrade from ICD to cardiac resynchronization therapy-defibrillator (CRT-D) with new RV and LV lead placement.
The left-sided cardiac device has been revised with the replacement of one of the LV leads and the placement of an additional lead which terminates at the coronary sinus.
There have been several reported cases in the medical literature of pacemaker leads becoming dislodged due to movement of the arm. This can occur when the lead is inserted through the subclavian vein, which is located near the collarbone, and the patient moves their arm in a way that causes the lead to become disconnected from the pacemaker.
One study from 2010 reported on a case of a patient with a dislodged pacemaker lead due to arm movement. The patient had a lead that had been inserted through the subclavian vein and connected to the pacemaker in the right chest [3]. When the patient moved their right arm, the lead became disconnected from the pacemaker, causing the heart to stop beating. The patient was able to reconnect the lead and restore normal heart function by holding the lead in place with their hand.
Another study reported on a case of a patient who developed a dislodged pacemaker lead due to repetitive arm movement. The patient had a lead that had been inserted through the subclavian vein and connected to the pacemaker in the left chest. The patient developed a dislodged lead due to repetitive arm movement, which caused the heart to stop beating [4]. The patient was able to restore normal heart function by reconnecting the lead and holding it in place with their hand.
A study published in the JAMA (Journal of the American Medical Association) found that the number of cases of unexpected lead failure was 1.13 per 100 patient years, which is still better than the old 4.41 per 100 patient years for the recalled lead (old generation leads) [5]. This study also found that the risk of lead fracture was higher for patients who had longer lead implantation times, had certain types of pacemaker leads, or had a history of chest trauma.
A study published in the Journal of Clinical Physiology and Functional Imaging found that the incidence of lead fracture among pacemaker patients was 0.21% per year [6]. This study also found that the risk of lead fracture was higher for patients with certain types of pacemaker leads and a history of chest trauma.
A study published in the Hindawi journal found that lead fractures occurred in 0.17% of pacemaker patients over a median follow-up of 5.8 years [7]. The study also found that the risk of lead fracture was higher for patients with certain types of pacemaker leads, had multiple leads implanted, had a history of chest trauma, or had longer lead implantation times. There have been several research papers that have reported evidence of pacemaker lead fracture. One study published in the Journal of the American Heart Association found that lead fractures occurred in 1.5% of pacemaker patients over a median follow-up period of 41 months [8]. The study also found that the risk of lead fracture was higher in patients who had leads that were inserted through the cephalic vein and in patients who had leads that were inserted using the “over-the-wire” technique, as opposed to the “through-the-sheath” technique.
Another study published in the Journal of Indian Pacing Electrophysiology found that lead fractures occurred in 3.2% of pacemaker patients over a median follow-up period of 69 months [9]. The study also found that the risk of lead fracture was higher in patients who had leads that were inserted through the cephalic vein and in patients who had leads that were inserted using the “over-the-wire” technique.
It is important to note that these cases are rare, and most pacemaker leads are stable and do not get dislodged with arm movement but can be fractured by any mechanical trauma or corrosion of the lead. According to the reviewed studies, the incidence of lead fracture among pacemaker patients is relatively low, with rates ranging from 0.13–0.3% per year. It is important that patients with pacemakers seek medical attention if they experience symptoms of a dislodged lead, such as sudden loss of consciousness or chest pain.
