Non-ST-Elevation Acute Coronary Syndrome and Predictors of Severity Coronary Artery Disease at the Oran University Hospital Center (Algeria)
Boukerche F1,2, Ali AA3,4*, and Hammou L1,2
1Department of Cardiology, Oran University Hospital Center, Oran, Algeria 2Faculty of Medicine, Oran, Algeria 3Department of Cardiology, Renaissance University Hospital Center, N’Djamena, Chad 4Faculty of Human Health Sciences of N’Djamena, N’Djamena, Chad
*Correspondence: Adam Ahamat Ali, Department of Cardiology, Renaissance University Hospital Center, N’Djamena, Chad
Received on 02 May 2020; Accepted on 29 May 2020; Published on 03 June 2020
Introduction: Non-ST-elevation (NSTE) acute coronary syndrome (ACS) is a common and polymorphic condition. Predicting significant coronary artery disease (CAD) is sometimes difficult. The objective of this study was to identify predictors of CAD severity in patients with non-ST-elevation acute coronary syndrome (NSTE-ACS). Patients and Methods: We prospectively evaluated 296 patients with NSTE-ACS who underwent a coronary angiography. Significant CAD was defined as ≥70% stenosis in at least one major coronary artery. Clinical characteristics in the hospital for 30 days and one-year outcomes were prospectively noted and a multivariate analysis was performed.
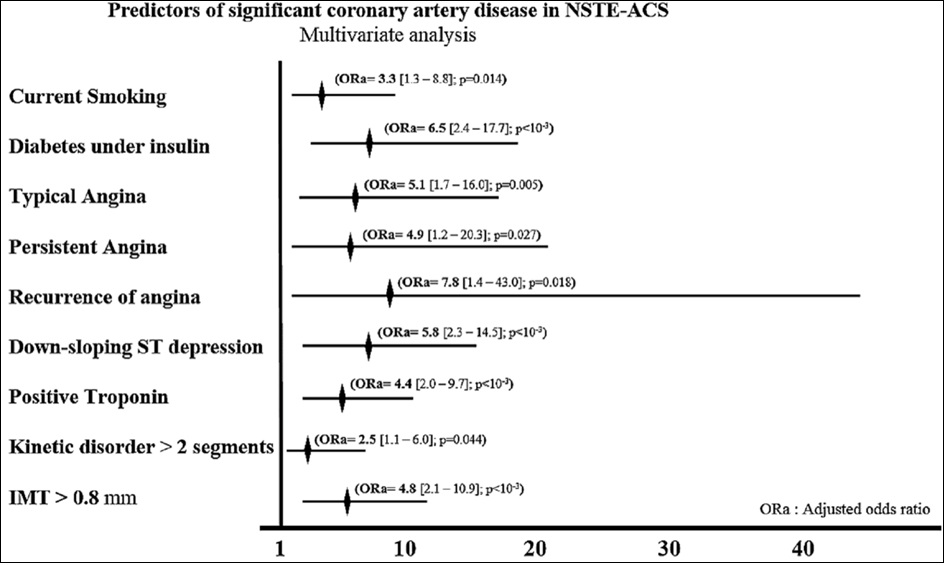
Results: The study included 296 NSTE-ACS patients. The mean age of the patients was 62.1 ± 12.6 years old while 58.1% of the patients were males. A multivariable analysis for the significant CAD predictors is shown (Figure 1), representing current smoking (ORa = 4.4; 95% confidence interval [CI] = 1.5–13.0, p = 0.007), a diabetic under insulin (Ora = 6.4; 95% [CI] = 2.4–17.4, p < 10-3), typical angina (ORa = 5.4; 95% [CI] = 1.7–16.8, p = 0.003), persistent angina (ORa = 5.3; 95% [CI] = 1.3–21.8, p = 0.019), recurrence of angina (ORa = 8.9; 95% [CI] = 1.5–51.4; p = 0.015), down sloping ST depression (ORa = 6.1; 95% [CI] = 2.4–15.3, p < 10-3), positive troponin (ORa = 4.2; 95% [CI] = 1.9–9.2, p < 10-3), kinetic disorder > 2 segments (ORa = 2.5; 95% [CI] = 1.1–6.0, p = 0.049), intima-media thickness (IMT) > 0.8 mm (ORa = 5.2; 95% [CI] = 2.3–12.1, p < 10-3). Conclusion: In this study, the severity of CAD was predicted by parameters such as typical or recurrent angina pectoris, current smoking, diabetic on insulin, down sloping ST depression, elevation of troponin, kinetic anomaly in more than two segments and the IMT greater than 0.8 mm.
Acute coronary syndrome (ACS) is a leading cause of death worldwide. The diagnosis and prediction of coronary artery disease (CAD) severity in non-ST elevation ACS (NSTE-ACS) with unstable angina and NSTE myocardial infarction, can be challenging. Cardiac biomarkers, electrocardiography, the symptoms, and cardiac risk factors are all used to diagnose NSTE-ACS [1] and make subsequent decisions on the need for invasive diagnostic studies. Despite risk stratification, 14% to 20% of patients undergoing cardiac catheterization are found to have normal or non-significant CAD [2, 3]. CAD is constantly increasing in our context. This is probably linked to the change in lifestyle of the population which favors the occurrence of chronic diseases such as diabetes and hypertension. The coronary angiography purpose in NSTE-ACS is to identify and revascularize significant CAD for the improvement of the outcome. A multitude of study groups have developed risk scores to assess patients’ risk of death or major adverse events [4–6]. The objective of this study was to identify predictors of CAD severity in patients with NSTE-ACS.
Patients and Methods
Study population
Patients were enrolled between November 01, 2015 and October 31, 2016 in the cardiology department located in Oran, north-west of Algeria. Patients aged ≥18 years who were admitted in the hospital with NSTE-ACS were eligible to participate. Those with symptoms precipitated by a secondary comorbidity (e.g., anemia, heart failure, and non-cardiac trauma) and patients who were participating in concomitant clinical trials were excluded. Significant stenosis is defined by narrowing ≥70% in at least one major coronary artery and 50% stenosis for the left artery main. Clinical characteristics in the hospital, a 30 day and a one-year outcome [major adverse cardiovascular and cerebrovascular events (MACCE)] have been studied. MACCE combined the end point of death, myocardial infarction and stroke. A one-year end point was the cause of death. This study has been approved by the management of the hospital, and all patients were provided with a signed informed consent.
Statistical analysis
Statistical analysis was performed in the 5% significant level, either using 2 sided tests’ or 2 sided CIs. Continuous data was given as the mean and range. Categorical data was summarized using counts and percentages. Logistic regression was performed to test the impact of covariates (e.g., patient characteristics, risk factors, Killip class, risk scores, cardiac biomarkers and angiographic finding) on outcome events. For this analysis, variables were selected as covariates based on a univariate analysis with a significant threshold of 0.20, and all the factors that were chosen in this selection process were included in a step-wise logistic regression model. For the final model, odds ratios and 95% care were given. Data were analyzed with the IBM SPSS Statistics 23. The results were expressed as mean ± standard deviation, percentages and tabulated. To compare the results, the proportional test for the relative risk calculation and the chi-square test (χ2) were used. The threshold of significance was set at p < 0.05.
Results
The study included 296 NSTE-ACS patients. The mean age of the patients was 62.1 ± 12.6 years old and 58.1% of the patients were males. 58.8% of the patients had a final diagnosis of NST-segment elevation myocardial infarction (NSTEMI).
208 patients had significant CAD and 78 non-significant CAD. Patients with significant CAD had a higher average age (63.3 vs. 58.7) and more often than not male, with a history of coronary artery disease, several cardiovascular risk factors (smoking, diabetes) and higher risk scores (GRACE, TIMI, heart) (Table 1). They had more recurrent and persistent angina, electrocardiogram ST depression and higher troponin levels (Table 2).
Predictors of significant coronary artery disease
Multivariable analysis for significant CAD predictors is shown (Figure 1), presenting currently smoking, diabetes mellitus under insulin, typical angina, persistent angina, recurrence of angina, downsloping ST depression, positive troponin, kinetic disorder > 2 segments at the echocardiography and IMT > 0.8 mm were correlated with significant CAD. Furthermore, we found that 24% (50/208) of patients with significant CAD had a low GRACE score on admission.
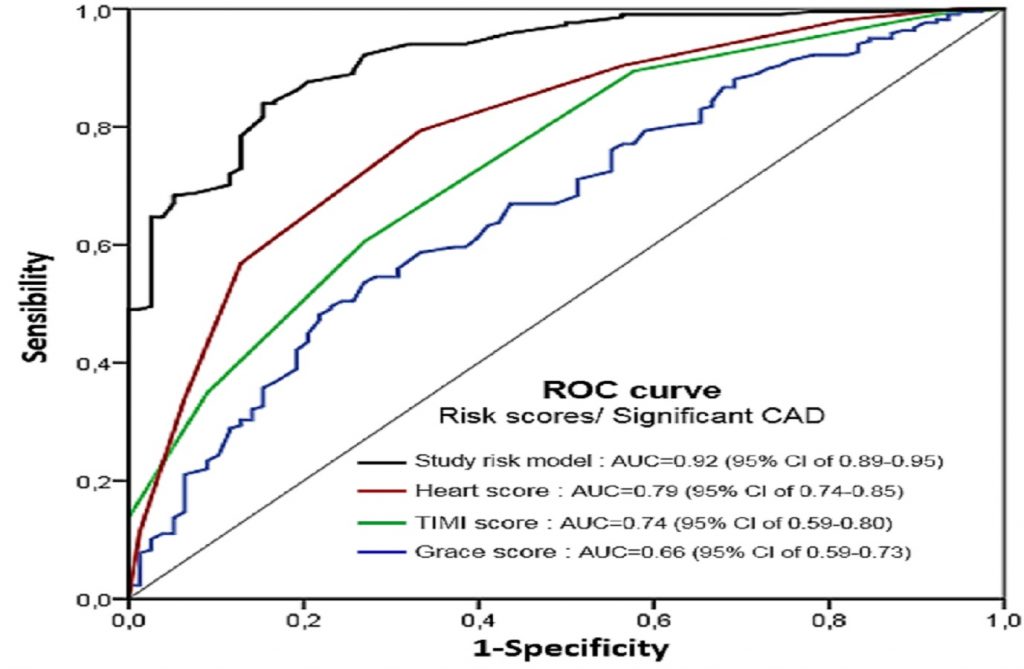
Using the ROC curve to compare the ability of the different risk scores (Grace, TIMI and heart scores) with our model risk score (from the multivariate analysis). This model of risk showed the highest concordance despite other risk scores followed by the heart score then TIMI and Grace score (Figure 2).
Patients with significant CAD had more hospital complications and a longer length of stay in the hospital. The 30 day to one-year follow-up showed a higher frequency of readmission rates, MACCE occurrence and mortality (Table 2).
Table 2: Electrocardiogram (ECG), laboratory test results and clinical outcomes. LVEF: left ventricular ejection fraction; WBC: white blood cells;
MACCE: major adverse cardiovascular and cerebrovascular events.
Figure 1: Multivariable analysis for predictors of significant CAD.
Figure 2: ROC curve to compare the ability of the different risk scores with our model risk score.
Comments
The main conclusions of this study were that the significant CAD in NSTE-ACS patients can be predicted by a set of clinical, cardiac, electrocardiographic and echocardiographic biomarker parameters. Thus, we identified 9 independent risk factors to predict the presence of a significant CAD: typical angina pectoris, recurrent angina pectoris, persistent angina pectoris, current smoking, insulin diabetes, positive troponin, ST depression downhill, kinetic disturbance in more than two segments and IMT at 0.8 mm. Among these factors, current smoking and insulin-dependent diabetes have the strongest correlation with significant CAD. At 30 days and one-year, patients with significant CAD have a higher mortality and complications rate than those who do not.
NSTE-ACS includes a clinical spectrum from unstable angina to NSTE myocardial infarction [7]. The pathophysiological mechanism is a rupture of the atherosclerotic plaque and different degrees of associated thrombosis and distal embolization [8, 9]. It is accompanied by a high mortality rate, hence the development of different risk scores (e.g., GRACE, TIMI, heart) by learned societies (ESC and ACC/AHA guidelines) to assess the risk of mortality and cardiovascular complications in order to define a precocious strategy (antithrombotic and invasive) and improve the prognosis. The early invasive strategy is recommended for high risk patients [10–13]. However, these scores are not established to predict significant CAD. In view of these data, some authors have sought to establish the link between the presence of significant CAD and clinical and paraclinical parameters [10, 14]. Beigel et al. [15] were able to identify, out of 2193 patients, 5 independent parameters (peripheral vascular disease, GRACE score of > 140, chronic renal failure, prior angina, and hyperglycemia on admission) predicting the coronary anatomy at high risk. Another study done by Patel et al. [14] revealed on the analysis of 215 patients that peripheral vascular disease, chronic renal failure and previous heart failure were independent predictors of significant CAD.
Although the scores remain important tools in practice for sorting patients at high risk for cardiovascular event(s), other elements are to be taken into account to identify important CAD as we showed our results and those of Beigel et al. [15]. The use of imaging tools as transthoracic echocardiography to evaluate LVEF (Simpson method), the heart segments kinetics and measuring of the IMT improve the risk assessment of NSTE-ACS patients.
Limitations
The study was conducted in one center with a small sample of patients. Further studies in the future seem necessary to arrive at results with greater reliability.
Conclusion
In this study, the severity of CAD was predicted by parameters such as typical or recurrent angina pectoris, current smoking, diabetic on insulin, down sloping ST depression, elevation of troponin, kinetic anomaly in more than two segments and the IMT greater than 0.8 mm.
Boukerche F, Ali AA, Hammou L. Non-ST-Elevation Acute Coronary Syndrome and Predictors of Severity Coronary Artery Disease at the Oran University Hospital Center (Algeria). Series Cardiol Res. 2020;2(1):3-9.