Abstract
Background: With the advancement of diagnostic modalities, there is an increase in the number of individuals detected with thyroid nodules. There are multiple treatment options for the management of nontoxic benign nodular goiter. Radioactive iodine results in effective goiter size reduction which can be administered as out-patient basis and is an appropriate alternative for patients with higher risk for surgery. Our group have shown the effectiveness of 131Iodine therapy for nodular nontoxic goiters. We aim to determine the long-term effectiveness of radioactive iodine therapy among patients with nodular nontoxic goiter.
Methods: This is a retrospective cohort study of patients with nontoxic benign nodular goiter, negative for malignancy on biopsy who underwent radioactive therapy with a follow-up of ≥36months using ultrasound studies. Thyroid size, number of nodules and size of nodules pre-treatment and ≥36months post-treatment were compared.
Results: 63 patients were included with an average follow-up of 73.14 ± 34.87 months. Mean age during radioactive therapy and last follow-up was 41 ± 14 and 47 ± 14 respectively. Significant thyroid size reduction was noted in 92.06% of patients (right thyroid lobe: 47.54 ± 31.25%, left thyroid lobe 47.44 ± 31.82%) while significant reduction in number and size of nodules were noted in 96.82% and 98.41% of patients respectively. No increase in the number of nodules and no development of new nodules were noted among all patients.
Conclusion: Radioactive iodine therapy for nontoxic benign nodular goiter produces a sustained reduction in thyroid size, number and size of nodules even after a long follow-up period. Hence, it is a viable alternative to surgical removal of the thyroid offering a lower risk for complication especially among patients who refuse surgery or has a contraindication to surgical management.
Keywords
131Iodine therapy, nodular goiter, nontoxic goiter, radioactive iodine, long-term follow-up
Abbreviations
TSH: thyroid stimulating hormone; RAI: radioactive iodine
Introduction
The incidence of benign thyroid nodules depends on mode of detection utilized. Palpation yields a prevalence of 5% while the use of ultrasonography increases the prevalence of thyroid nodule to as high as 50% among individuals more than 50 years of age [1]. Without treatment, goiters may remain stable or progressively increase in size or develop multiple nodules rendering the patient to experience symptoms such as dysphagia or dyspnea [2].
Multiple options are available for the treatment of nontoxic benign nodular goiter. Suppression therapy with the use of levothyroxine suppresses thyroid stimulating hormone (TSH) level inhibiting further increase in the size of the thyroid nodule as well as the thyroid gland itself. Studies showed that treatment with a combination of iodine and levothyroxine suppression therapy reduces the thyroid nodule volume and the thyroid gland volume. The noted reduction in thyroid nodule and thyroid gland size is lost once therapy is discontinued. It also carries the risk of iatrogenic subclinical hyperthyroidism which adversely affects the skeleton and the cardiovascular system [3–6].
Surgical removal of the thyroid gland has been commonly used and causes complete and rapid removal of the goiter but it carries the risk for both surgical and anesthetic complications such as injury to the recurrent laryngeal nerve, trachea or parathyroid glands [4]. There are several surgical options for removal of thyroid including lobectomy, bilateral subtotal thyroidectomy, total thyroidectomy and hemithyroidectomy with contralateral subtotal resection known as the Dunhill operation. A more aggressive approach was found to have a lower rate of recurrence but with a higher rate of complication [7, 8]. In a study conducted among Filipino patients who underwent unilateral lobectomy for the management of nodular nontoxic goiter, recurrence of benign thyroid nodule after 16 ± 10 years was noted with majority of recurrence occurring after 1–10 years [9]. In another study, 14.7% of patients who underwent lobectomy required reoperation because of recurrence [10]. A more recent study comparing total thyroidectomy, bilateral subtotal thyroidectomy and the Dunhill operation showed a lower recurrence of goiter after 10 years among patients who underwent total thyroidectomy. Recurrence was noted in 0.6% patients after total thyroidectomy while recurrence was noted in 8.6% and 22.4% of patients who underwent the Dunhill operation and bilateral subtotal thyroidectomy respectively. Some of the patients with recurrence required revision thyroidectomy and the less than total thyroid resections were found to have a higher incidence of revision thyroidectomy as compared to total thyroidectomy. Similar to other studies, they found that total thyroidectomy was associated with a higher risk of complication and revision thyroidectomy has an even higher risk for complication compared to the initial surgical procedure [11].
The use of radioactive iodine for benign nontoxic goiter has been introduced for more than 20 years. Multiple studies have noted an effective reduction in thyroid volume after radioactive iodine therapy with greatest size reduction during the first 3 months after treatment [12–15]. Its advantages include an effective goiter reduction which can be administered as out-patient making it more cost-effective compared to surgical procedures. It is also an appropriate choice for patients with a higher risk for surgery and anesthesia [5, 12, 16].
A number of studies recommended the use of recombinant human thyrotropin as pre-stimulation prior to radioactive iodine therapy for patients with nontoxic benign nodular goiter because of a greater reduction in thyroid volume as compared to radioactive iodine therapy alone [17–20]. However, several studies in the Philippines have shown similar success in goiter and benign nodule reduction even without the use of recombinant human thyroid-stimulating hormone. A study by Atanacio et al. and Abcede et al. among Filipino patients with diffuse or nodular nontoxic goiter showed reduction in thyroid size as well as reduction in the mean nodule size after radioactive iodine therapy without the aid of recombinant human thyroid-stimulating hormone. An associated clinical improvement with a reported relief of neck discomfort and choking sensation was noted [21]. Given the nodule size reduction and symptomatic relief documented, this study supports the use of radioactive iodine therapy in nontoxic benign nodular goiter as an effective and safer alternative. However, there is no available local data on the sustainability of nodule size reduction as well as the risk of recurrence among patients who underwent radioactive iodine therapy for patients with nontoxic benign nodular goiter. It is therefore the objective of this study to describe the long-term (> 36 months) effect of radioactive iodine therapy in nontoxic benign nodular goiter.
Materials and Methods
Study design and patients
This study was carried out in accordance with the applicable International Conference on Harmonization Guidelines on Good Clinical Practice Guidelines and was conducted upon approval by the UST Hospital Institutional Review Board who waived the requirement for informed written consent. All patient information and records included in the study were held in strict confidence.
This is a retrospective cohort study of patients with nontoxic benign nodular goiter. Patients were selected from an endocrine specialty clinic from January 2000 to December 2014. This study involved patients, aged 18 years and above, with nodular nontoxic goiter with a benign histopathology report from a fine needle aspiration biopsy treated with radioactive iodine therapy who came for follow-up at least 36 months after the administration of radioactive iodine. Patients who failed to follow-up 36 months after radioactive iodine therapy and those who underwent total thyroidectomy were excluded.
Charts and medical records of patients who fulfilled the inclusion criteria were retrieved and reviewed. The following parameters at least 36 months post-therapy were assessed: number of nodules, size of previously documented nodules, new nodule formation and latest dose of levothyroxine.
Data analysis
Pertinent data including demographic characteristics, baseline thyroid hormone levels, ultrasound characteristics and histopathologic report were recorded. Thyroid size, nodule size, number of nodules pre-therapy and at least 36 months after therapy were recorded and compared. New nodule formation as well as the latest TSH level and dose of levothyroxine were also recorded. Percentage of patients with sustained decrease in number of nodules and size reduction of nodules and the percentage of patients with new nodule formation among patients with nodular nontoxic goiter after radioactive iodine therapy were computed. Microsoft Excel version 2016 was used for data analysis.
Results
A total of 63 patients were included in this study, of which 97% were women. The table shows the general features of patients included in the study (Table 1). Mean age during radioactive iodine therapy was 41 years and mean age at the time of last follow-up was 47 years. Follow-up period ranged from 36–168 months with a mean of 73.14 ± 34.87 months.
Mean size of the right thyroid lobe and left thyroid lobe prior to treatment was 8.04 ± 3.73 cm2 and 7.65 ± 2.70 cm2. Mean number of nodules prior to treatment was 1.67 ± 1.09 with the largest nodule at 2.13 ± 1.65 cm2 and the smallest nodule at 0.48 ± 0.97 cm2.
Mean dose of radioactive iodine received was 13.75 ± 4.65 mCi. Most of the patients (76.19%) received a single dose of radioactive iodine therapy while a few of the patients received 2 (22.22%) or 3 doses (1.59%) of radioactive iodine therapy.
There was a significant decrease in the size of the right (p = 0.00) and left (p = 0.00) thyroid lobe, number of nodules (p = 0.00) as well as in the size of largest (p = 0.00) and smallest (p = 0.01) nodules on follow-up at least 36 months post-radioactive iodine therapy (Figure 1) (Table 2). Right and left thyroid lobe size were reduced by 47.54 ± 31.25% and 47.44 ± 31.82% respectively. Number of nodules decreased with a computed percent reduction of 94.29 ± 19.73%. The size of the largest nodule was reduced by 88.98 ± 48.05% while the size of the smallest nodule was reduced by 33.33 ± 47.52%.
| N = 63 | Mean ± SD/Percentage (95% CI) |
| Duration of follow-up (months) | | 73.14 ± 34.87 (64.36 – 81.92) |
| Age at the time of 131I-therapy (years) | | 41±14 (37.74 – 44.87) |
| Age at the time of last follow-up (years) | | 47±14 (43.79 – 50.98) |
| Dose of RAI (mCi) | | 13.75 ± 4.65 (12.58 – 14.92) |
| Sex | Female | 97% |
| Male | 4% |
| Right thyroid lobe size (cm2) | Pre-treatment | 8.04 ± 3.73 (7.10 – 8.98) |
| ≥36months post-treatment | 3.57 ± 1.74 (3.13 – 4.00) |
| Left thyroid lobe size (cm2) | Pre-treatment | 7.65 ± 2.70 (6.97 – 8.33) |
| ≥36months post-treatment | 3.62 ± 1.62 (3.22 – 4.03) |
| Number of nodules | Pre-treatment | 1.67 ± 1.09 (1.39 – 3.06) |
| ≥36months post-treatment | 0.13 ± 0.38 (0.03 – 0.22) |
| Size of largest nodule (cm2) | Pre-treatment | 2.13 ± 1.65 (1.72 – 2.55) |
| ≥36months post-treatment | 0.37 ± 1.72 (-0.07 – 0.80) |
| Size of smallest nodule (cm2) | Pre-treatment | 0.48 ± 0.97 (0.24 – 0.72) |
| ≥36months post-treatment | 0.11 ± 0.85 (-0.11 – 0.32) |
| TSH (uIU/mL) | Pre-treatment | 1.46 ± 1.37 (1.12 – 1.81) |
| ≥36months post-treatment | 5.53 ± 9.83 (3.06 – 8.01) |
| Levothyroxine dose on last follow-up (ug/day) | | 81.44 ± 27.90 (74.42 – 88.47) |
Table 1: Clinical profile of patients with nontoxic benign nodular goiter who underwent 131I-therapy.
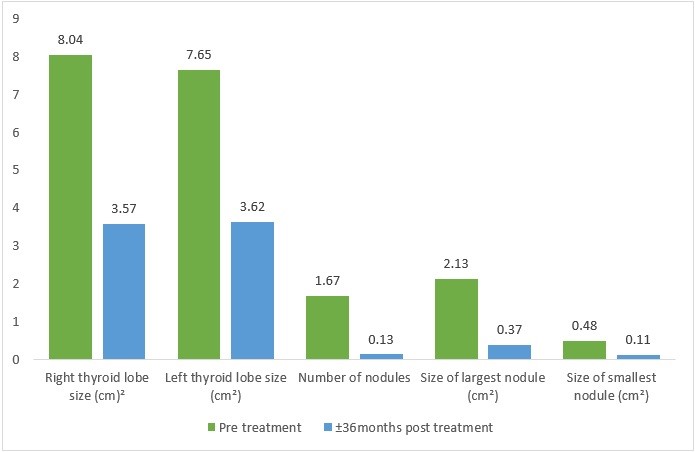
Figure 1: Reduction in the right and left thyroid size, number of nodules and size of largest and smallest nodule pre-treatment and ± 36 months post-treatment.
| N = 63 | p value | % reduction (mean ± SD) (95% CI) |
| Right thyroid lobe size (cm2) | Pre-treatment | 8.04 ± 3.73 | 0.00 | 47.54 ± 31.25 (39.67 – 55.42) |
| ≥36months post-treatment | 3.57 ± 1.74 |
| Left thyroid lobe size (cm2) | Pre-treatment | 7.65 ± 2.70 | 0.00 | 47.44 ± 31.82 (39.43 – 55.45) |
| ≥36months post-treatment | 3.62 ± 1.62 |
| Number of nodules | Pre-treatment | 1.67 ± 1.09 | 0.00 | 94.29 ± 19.73 (89.32 – 99.26) |
| ≥36months post-treatment | 0.13 ± 0.38 |
| Size of largest nodule (cm2) | Pre-treatment | 2.13 ± 1.65 | 0.00 | 88.98 ± 48.05 (76.88 – 101.08) |
| ≥36months post-treatment | 0.37 ± 1.72 |
| Size of smallest nodule (cm2) | Pre-treatment | 0.48 ± 0.97 | 0.01 | 33.33 ± 47.52 (21.37 – 45.30) |
| ≥36months post-treatment | 0.11 ± 0.85 |
Table 2: Comparison between thyroid size, nodule number and size in the pre-treatment period and ≥36 months post-treatment with percent reduction.
Among the 63 patients included in the study, 92.06% demonstrated sustained reduction in thyroid size. Complete disappearance of nodules was noted in 88.89% of patients while 96.82% of patients were noted to have a sustained decrease in the number of nodules. No increase in the number of nodules was noted among all patients. In addition, 98.41% of patients revealed a sustained decrease in the size of nodules post-therapy with radioactive iodine.
Discussion
In previous studies conducted, they were able to note a significant reduction in thyroid size and nodule size after radioactive iodine therapy [2, 14, 15]. Similar to other studies, we were also able to demonstrate a significant reduction in the size of the thyroid and size of the nodules. Compared to the study conducted by Sia-Atanacio et al. [2], wherein they documented a 29.32% decrease in thyroid size and a 38% reduction in nodule size after radioactive iodine therapy after a mean follow-up of 3.57 ± 3.47 months, we were able to document a higher percent reduction in thyroid size of 47%. Our documented decrease in nodule size was also higher at 89% for the largest nodule and 33% for the smallest nodule. Our documented thyroid size reduction was comparable to the study done by Kaniuka-Jakubowska et al. [14] wherein a thyroid size reduction of 43% after 12 months was reported. In another study by Nygaard et al. [16], they noted a median 60% reduction in thyroid size after 12 months which is higher than our documented reduction in thyroid size. Similarly, the study done by Heydari et al. [15] recorded a higher thyroid size reduction at 77.8% after a follow-up of 2 years. However, their documented reduction in thyroid nodule size of 40% on average was lower to our documented reduction in the size of the largest nodule but was comparable to our noted reduction in the size of the smallest nodule.
Compared to previous studies wherein they were unable to document a change in the number of nodules after radioactive iodine therapy, we were able to document a 94% reduction in the number of nodules among patients with benign nodular nontoxic goiter. In addition, our study has a longer period of follow-up at 73.14 ± 34.87 months with a range of 36–168 months compared to other studies which had a mean follow-up period of less than 24 months.
Contrary to the study by Barczynski et al. [11] wherein recurrence was noted despite surgical removal of the thyroid with number of patients requiring revision thyroidectomy, our study noted a sustained decrease in the number and size of nodules. Formation of new nodules was also absent during this long period of follow-up. This reinforces the sustained beneficial effects of radioactive iodine therapy among patients with nontoxic benign nodular goiter proving that the use of radioactive iodine therapy for nontoxic benign nodular goiter has a long-term effect in the reduction of thyroid size, number of nodules and nodule size. In addition, compared to surgical removal of the thyroid, radioactive therapy has a lower risk for complications and may offer a shorter hospital stay, faster recovery from the procedure as well as lower cost of treatment. Hence, it is a viable alternative especially among patients who refuse surgery or has a contraindication to surgical management.
The major strength of this study is its longer follow-up period compared to similar studies which allowed an observation for the long-term effectiveness of radioactive iodine therapy on nontoxic benign nodular goiter. On the other hand, our study did not include patients with very large goiters and thus cannot be used in the decision-making for patients with very large goiters who refuse or cannot undergo surgery.
Conclusion
Radioactive iodine therapy for nontoxic benign nodular goiter produces a sustained reduction in thyroid size, number and size of nodules even after a long follow-up period. Hence, it is a viable alternative to surgical removal of the thyroid offering a lower risk for complication especially among patients who refuse surgery or has a contraindication to surgical management.
Conflicts of Interest
We have no conflicts of interest to disclose.
Funding Statement
This study was completed without external funding or grants.
Acknowledgement
References
- Bahn RS, Castro MR. Approach to the patient with nontoxic multinodular goiter. J Clin Endocrinol Metab. 2011;96(5):1202-12.
- Sia-Atanacio A, Mercado-Asis L. Radioactive iodine therapy is effective in diffuse and nodular nontoxic goiter. Phil J Internal Medicine. 2011;49(2):70-73.
- Uy J, Mercado-Asis L. Prevention of recurrence of diffuse and nodular nontoxic goiter with lifetime physiologic levothyroxine maintenance therapy. Phil J Internal Medicine. 2009;47(1):207-10.
- Bonemma S, Fast S, Hegedus L. Non-surgical approach to the benign nodular goiter: new opportunities by recombinant human TSH-stimulated 131I-therapy. Endocrine. 2011;40(3):344-53.
- Wesche M, Buul M, Lips P, et al. A randomized trial comparing levothyroxine with radioactive iodine in the treatment of sporadic nontoxic goiter. J Clin Endocrinol Metab. 2001;86(3):998-1005.
- Puzziello A, Carrano M, Angrisani E, et al. Evolution of benign thyroid nodules under levothyroxine non-suppressive therapy. J Endocrinol Invest. 2014;37(12):1181-186.
- Mauriello C, Marte G, Canfora A, et al. Bilateral benign multinodular goiter: what is the adequate surgical therapy? A review of literature. Int J Surg. 2016;28(Suppl 1):S7-S12.
- Rayes N, Seehofer D, Neuhaus P. The surgical treatment of bilateral benign nodular goiter: balancing invasiveness with complications. Dtsch Arztebl Int. 2014;111(10):171-78.
- Udarbe P, Mercado-Asis L, Lim W, et al. Recurrence of benign solitary thyroid nodule after a unilateral lobectomy. Phil J Internal Medicine. 2006;44(3):135-39.
- de Rienzo-Madero B, Sabra J, Gand E, et al. Unilateral benign multinodular versus solitary goiter: Long-term contralateral reoperation rates after lobectomy. Surgery. 2018;165(1):75-79.
- Barczynski M, Konturek A, Hubalewska-Dydejczyk A, et al. Ten-year follow-up of a randomized clinical trial of total thyroidectomy versus Dunhill operation versus bilateral subtotal thyroidectomy for multinodular non-toxic goiter. World J Surg. 2018;42(2):384-92.
- Feldt-Rasmussen U. Radioiodine treatment for non-toxic goitre. F1000 Med Rep. 2009;1:70.
- Paz-Filho G, Mesa-Junior C, Olandoski M, et al. Effect of 30 mCi radioiodine on multinodular goiter previously treated with recombinant human thyroid-stimulating hormone. Braz J Med Biol Res. 2007;40(12):1661-670.
- Kaniuka-Jakubowska S, Lewczuk A, Mizan-Gross K, et al. Large multinodular goiter–outpatient radioiodine treatment. Endokrynol Pol. 2015;66(4):301-07.
- Heydari I, Honardoost M, Moradi S, et al. Changes in the size of the thyroid in patients with benign non-toxic multinodular goiter after radioactive iodine therapy. Med J Islam Repub Iran. 2018;32:131.
- Nygaard B, Hegedus L, Gervil M, et al. Radioiodine treatment of multinodular non-toxic goitre. BMJ. 1993;307(6908):828-32.
- Fast S, Nielsen V, Grupe P, et al. Prestimulation with recombinant human thyrotropin (rhTSH) improves the long-term outcome of radioiodine therapy for multinodular nontoxic goiter. J Clin Endocrinol Metab. 2012;97(8):2653-660.
- Albino C, Graf H, Paz-Filho G, et al. Radioiodine plus recombinant human thyrotropin do not cause acute airway compression and are effective in reducing multinodular goiter. Braz J Med Biol Res. 2010;43(3):303-09.
- Bonnema S, Nielsen V, Boel-Jorgensen H, et al. Improvement of goiter volume reduction after 0.3 mg recombinant human thyrotropin-stimulated radioiodine therapy in patients with a very large goiter: a double-blinded, randomized trial. J Clin Endocrinol Metab. 2007;92(9):3424-428.
- Nielsen V, Bonnema S, Boel-Jorgensen H, et al. Stimulation with 0.3-mg recombinant human thyrotropin prior to iodine 131 therapy to improve the size reduction of benign nontoxic nodular goiter: a prospective randomized double-blind trial. Arch Intern Med. 2006;166(14):1476-482.
- Abcede A, Kho S, Matawaran B, et al. Successful reduction in thyroid and nodule volumes in large solitary and multinodular goiters with serial 131iodine therapy. Phil J Internal Medicine. 2017;55(4):1-5.
