Laaouina S *, Saidi S, Oubaaz B, Elkhouyaali A, Fiqhi A, Mouzari Y and Oubaaz A
*, Saidi S, Oubaaz B, Elkhouyaali A, Fiqhi A, Mouzari Y and Oubaaz A
Department of Ophthalmology, Mohammed V Military Hospital of Rabat, Mohammed V University, Rabat, Morocco
*Corresponding author: Soukaina Laaouina, Department of Ophthalmology, Mohammed V Military Hospital of Rabat, Mohammed V University, Rabat, Morocco
Received: 29 October 2024; Accepted: 02 December 2024; Published: 04 December 2024
© 2024 The Authors. This is an open-access article and is distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Abstract
Essential thrombocythemia (ET) is a rare chronic myeloproliferative disorder characterized by significant thrombocytosis. The ocular manifestations reported during ET are rare and are mainly represented by occlusion of the central retinal vein. We present the case of a 67 years old patient who was referred for an acute visual loss in the right eye, without associated pain or redness, and whose clinical examination on the admission found vitreous hemorrhage of the right eye, associated with microhyphema and ocular hypertonia. The pre-therapeutic biological assessment revealed hyperplateletosis at 1,146,000/mm3, without associated myelemia. The patient was treated with general and topical hypotonizing treatment, and was referred after the normalization of his intraocular pressure (IOP) to hematology for further management. The assessments carried out were in favor of ET and cytoreductive treatment was initiated. Ophthalmological involvement during ET is rare. This is the first case of spontaneous vitreous hemorrhage as an ocular complication of ET.
Keywords
glaucoma, vitreous hemorrhage, essential thrombocythemia
Abbreviations
ET: essential thrombocythemia, IOP: intraocular pressure
Introduction
Essential thrombocythemia (ET) is a rare chronic myeloproliferative disorder characterized by significant thrombocytosis. It is usually diagnosed in the sixth decade of life, and more commonly affects females. It is often asymptomatic, but vascular occlusive events include thromboses of large arteries and veins, and microvessels, generate neurological, cardiac, or peripheral arterial disabilities [1]. The incidence of hemorrhagic complications is relatively exceptional [2].
The ocular manifestations reported during ET are rare and are mainly represented by occlusion of the central retinal vein.
We report the case of a patient who presents with secondary ocular hypertonia associated with vitreous hemorrhage, in whom pre-therapeutic assessment revealed the presence of ET.
Case Report
We present the case of a 67-year-old patient with no significant medical history, referred to the ophthalmology department due to acute visual loss in the right eye, without associated pain or redness. The patient did not report any history of ocular trauma.
Upon admission, clinical examination revealed reduced visual acuity in the right eye, limited to hand movements, while the left eye maintained a visual acuity of 9/10 (as tested on the Snellen chart). Examination of the anterior segment of the right eye showed corneal edema and a deep anterior chamber containing microhyphema. The iris appeared normal, with no signs of iris rubeosis, and the pupil was round with a preserved photomotor reflex and intraocular pressure (IOP) of the right eye was 58 mmHg.
Fundus examination was not possible due to dense vitreous hemorrhage, classified as grade 3. Gonioscopy of the right iridocorneal angle revealed an open angle, with a blood clot present in the lower and nasal quadrants (Figure 1). The examination of the left eye was unremarkable.
B-mode ultrasound of the right eye indicated intravitreal hemorrhage, with the retina appearing flat and no visible tears (Figure 2).
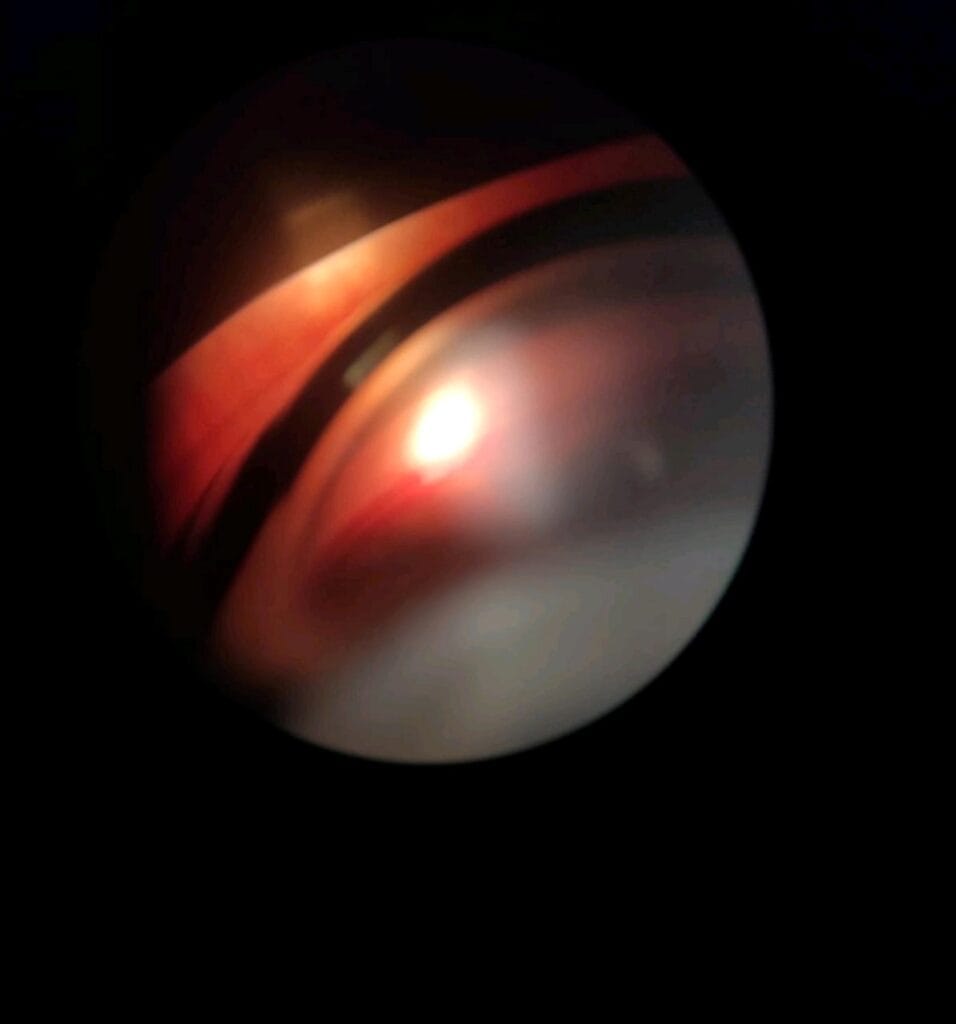 Figure 1: Stigma of blood in the iridocorneal angle.
Figure 1: Stigma of blood in the iridocorneal angle.
 Figure 2: B-scan ultrasound of the right eye showing a massive vitreous hemorrhage.
Figure 2: B-scan ultrasound of the right eye showing a massive vitreous hemorrhage.
The pre-therapeutic biological assessment showed hyperplateletosis at 1,146,000/mm3, without associated myelofibrosis.
The patient was treated with general and topical hypotensive medications. After normalization of IOP, he was referred to hematology for further management.
During hospitalization, an osteomedullary biopsy was performed, which showed hyperplasia of the megakaryocytic lineage without tumor infiltration. Testing for JAK2, CALR, and MPL mutations returned negative results. A diagnosis of ET was established, and treatment with cytoreductive therapy was initiated.
The patient was proposed for a later vitrectomy following the management of his hyperplateletosis.
Discussion
ET is a rare hematological disease that can remain asymptomatic for significant periods. It is frequently discovered incidentally during platelet counts or revealed through serious thrombotic or hemorrhagic complications. This condition predominantly affects middle-aged adults [3].
The diagnostic criteria for ET are clear: a persistent hyperplateletosis, with counts ranging from 450 to over 2,000 g/L, must be present, alongside the absence of other causes for hyperplateletosis, such as inflammatory syndromes, iron deficiency, or hypersplenism [4].
Hemorrhaging in ET arises from defective platelet function, which hinders the formation of a red thrombus necessary to seal a vascular breach, resulting in hypoaggregability [5, 6]. The bleeding complications commonly associated with ET are indicative of platelet and vascular disorders. Patients typically experience bruising, epistaxis, and superficial mucosal hemorrhages (e.g., gastrointestinal, genitourinary, and gingival). Deep tissue and visceral bleeding (e.g., hemarthrosis, retroperitoneal hemorrhage) are exceedingly rare. Importantly, there is no direct correlation between platelet count and the occurrence of hemorrhage [7].
Ophthalmological involvement in ET is uncommon but significant. It can result from thrombotic complications that lead to occlusion of the central retinal artery or vein, or from retinal embolism due to a platelet thrombus.
Currently, there is no curative treatment for ET. Management efforts are vital, focusing on preventing thrombo-hemorrhagic complications and minimizing the risk of hematological progression, thus enhancing patients’ quality of life. The treatment strategy primarily includes cytoreductive therapies designed to reduce thrombocytosis. The use of antiplatelet agents is not recommended due to the heightened risk of bleeding; in our patient, these were contraindicated because of existing vitreous hemorrhage [8].
Conclusion
Ocular complications of ET are rare and serious since they can threaten visual function. Luckily, early diagnosis, recognition, and appropriate treatment lead to the stabilization of the disease, which allows the prevention or control of complications.
Conflicts of Interest
The authors declare they have no conflict of interest.
References
- Billot S, Kouroupi EG, Le Guilloux J, et al. Neurological disorders in essential thrombocythemia. Haematologica. 2011;96(12):1866-869.
- Brière JB. Essential thrombocythemia. Orphanet J Rare Dis. 2007;2:3.
- Michiels JJ, Thiele J. Clinical and pathological criteria for the diagnosis of essential thrombocythemia, polycythemia vera, and idiopathic myelofibrosis (agnogenic myeloid metaplasia). Int J Hematol. 2002;76(2):133-45.
- Walsh PN, Murphy S, Barry WE. The role of platelets in the pathogenesis of thrombosis and hemorrhage in patients with thrombocytosis. Thromb Haemost. 1977;38(4):1085-096.
- Thabsuwan K, Chantarasorn Y. Essential thrombocythemia manifesting as ophthalmic artery occlusion. Am J Ophthalmol Case Rep. 2020;18:100724.
- Asensio Sánchez VM, Manteca Jiménez G, Cano Navarro E. Essential thrombocythemia and retinal vein thrombosis. Arch Soc Esp Oftalmol. 2004;79(12):629-32.
- Singer G. Migrating emboli of retinal arteries in thrombocythaemia. Br J Ophthalmol. 1969;53(4):279-81.
- Tefferi A, Vannucchi AM, Barbui T. Essential thrombocythemia treatment algorithm 2018. Blood Cancer J. 2018;8(1):2.
