Pilonidal sinus is a common disease of the sacrococcygeal region. The pilonidal sinus of the umbilicus is not frequently reported in the literature. The disease having an atypical presentation is often misdiagnosed. The presenting symptoms include pain and discharge. There is no consensus regarding the treatment hence, both conservative treatment and surgery have been suggested for the management of the disease. We present a case of umbilical pilonidal sinus (UPS), which was managed surgically after the conservative trial of management had failed. We have also discussed the current review of literature regarding the management of this rare clinical disorder.
umbilical pilonidal sinus, sacrococcygeal pilonidal sinus, computerized tomography
UPS: umbilical pilonidal sinus, CT: computerized tomography
Pilonidal sinus is a common chronic disorder characterized by the formation of a sinus lined with granulation tissue. The disease, although commonly involving the sacrococcygeal region, may be encountered in other parts of the body, such as the web space of fingers, axilla, perineum, penile shaft, amputation stump, and umbilicus. The incidence of the umbilical pilonidal sinus (UPS) is about 0.6% of all cases of pilonidal disease. Pain and discharge from the umbilicus are common presenting symptoms of UPS, while erythema and tenderness suggest a complicated disease. The conservative treatment includes hair removal, maintaining hygiene, and drainage of abscess, while surgical management is by excision of the sinus with the umbilicus.
An 18-year-old gentleman presented with recurrent intermittent discharge from the umbilicus for 3 months, which was serosanguineous in nature. There was no history of any fever, any obvious trauma to the umbilicus, or an increase in the discharge during micturition. The physical examination revealed a hirsute male with a deep umbilicus. Mild erythema around the umbilicus was present, serosanguineous discharge was present from the umbilical cicatrix, and a detailed examination of the umbilicus demonstrated a tuft of hair with granulation tissue (Figure 1).
The patient was given a trial of an antibiotic course and anti-inflammatory agents and was advised to maintain hygiene along with regular depilation around the umbilicus. The inflammation and discharge subsided with the conservative treatment; however, he had a recurrence of the symptoms after a month. A computerized tomography (CT) sinogram was done to rule out urachal anomalies or any omphalomesenteric anomaly. CT sinogram revealed a superficial fistula without any intra-abdominal communication. The umbilical-urachal sinus was normal in caliber (Figure 2).
In view of the failure of conservative management, the patient was taken up for exploration under anesthesia. Intra-operative findings revealed a sinus with pinkish granulation tissue and a tuft of hair embedded in the sinus. The sinus didn’t have any intra-peritoneal communication. Excision of the sinus along with the umbilicus was done, and neo-umbilicus was created. The post-operative period was uneventful. The histopathological examination of the excised specimen revealed keratinized stratified squamous epithelium with underlying lymphoplasmocytic inflammatory infiltrate and areas of fibrosis (Figure 3). The patient has been advised to maintain personal hygiene with regular depilation around the umbilicus, and after one year of follow-up, has no evidence of any recurrence of the disease.
 Figure 1: Picture demonstrating a deep naval with a tuft of hair with the granulation tissue extracted from the umbilicus (arrow).
Figure 1: Picture demonstrating a deep naval with a tuft of hair with the granulation tissue extracted from the umbilicus (arrow).
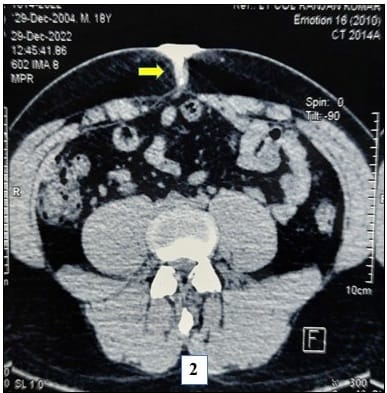
Figure 2: CT sinogram demonstrating a superficial fistula (arrow) with no communication of the contrast with the peritoneal cavity.

Figure 3: Histopathological examination of the excised specimen showing keratinized stratified squamous epithelium with underlying lymphoplasmocytic infiltrates.
Pilonidal sinus disease is a chronic disorder that is characterized by the formation of the sinus with granulation tissue due to penetration of the epidermis with a hair shaft. While the term pilonidal sinus was coined in 1880 by Hodges, the first case of pilonidal sinus was reported by Patey and Williams in 1956 [1–4]. The disease has significant morbidity and is associated with substantial social impact.
3.1 Prevalence and characteristics
The sacrococcygeal region is the most common location involved by the pilonidal sinus. The less frequently involved body parts include the web space of fingers, axilla, perineum, penile shaft, amputation stump, and umbilicus [2, 5–7]. The spectrum of pilonidal disease includes pilonidal sinus, pilonidal cyst, and pilonidal abscess [3, 5, 7]. UPS is an uncommon disease with an incidence of around 0.6% of all cases of pilonidal disease and only a few 100 cases mentioned in the literature [3, 5, 7].
3.2 Aetiopathogenesis
There are two theories about the etiology of pilonidal sinus – the developmental theory and the acquired theory. As per the developmental theory, there are epidermal rests with hair embedded below the dermis in the midline resulting from failure of fusion. The acquired theory suggests that the distal end of the shed hair around the affected region penetrates into the small sebaceous or hair follicles. This facilitates the penetration of the hair into the dermis and subcutaneous tissue, creating minute pits, which subsequently get infected by skin organisms, causing suppuration [8]. The absence of hair follicles and the uniform orientation of hairs, with the roots directed towards the end of the sinus tract in most specimens, support the theory of an acquired condition over a congenital cause [1, 2, 5, 7, 9]. It has been postulated that the hair shed from the chest and abdomen is pulled into the umbilical orifice by the tugging action of the unobliterated urachus. The hairs caught in the umbilicus puncture the umbilical recess, which triggers a foreign body inflammatory reaction resulting in further narrowing of the umbilical orifice due to the resulting edema. An abscess may form following a local infection [10–13].
3.3 Predisposing factors
The predisposing factors for UPS include male sex, young age, hairiness, a deep navel, and poor personal hygiene. Although the sacrococcygeal pilonidal sinus is more common in obese patients, it is uncommon in UPS. This is due to a decrease in migration of the hair to the umbilical recess resulting from the flattening of the umbilical hole in obese patients [10–13].
3.4 Clinical signs and symptoms
The presenting complaint of the patients with UPS includes pain and sanguineous or purulent discharge from the umbilicus. Local tenderness and erythema may be present and indicate abscess formation. The disease is often misdiagnosed and mistreated before a definitive diagnosis is made due to the rarity of the disease [5, 11, 14]. The differential diagnosis of UPS includes umbilical hernia, metastatic tumors like Sister Mary Joseph nodule, omphalomesenteric duct remnants (Meckel’s diverticulum), urachal anomalies, endometriosis in women and nevi [3, 10, 15].
3.5 Treatment – conservative vs operative management
The treatment of UPS includes both conservative management and surgery. The conservative management of UPS includes maintaining strict hygiene, removing the tuft of hair, antibiotics, curettage of the cavity, drainage of abscess, silver nitrate application for granulomas, and depilation or shaving of the hairs around the umbilicus to prevent the recurrence [3, 16–18]. The surgical intervention includes complete excision of the sinus with or without reconstruction, umbilectomy and primary repair, incision and curettage, umbilectomy and secondary closure of the wound with subsequent scar resembling a normal umbilicus [19]. The proponents of conservative management believe that the excision of the umbilicus is not warranted as the disease is congenital in origin [10, 16–18].
UPS is a very rare umbilical disorder usually associated with significant morbidity and social impact. There are several risk factors for the disease, and the common manifestations of the disease include pain and discharge from the umbilicus. Most of the cases can be managed conservatively, with surgery indicated in case of failure of the conservative therapy.
