Abstract
Background: Premenstrual syndrome (PMS) causes a variety of disturbing symptoms that can affect mood, cognition, and physical well-being and have effects on the regular lives of females, especially students.
Objective: Assessment of female students’ knowledge, attitude, and awareness regarding PMS, evaluation of the prevalence of PMS in Bangladesh, and its impact on the regular life of female students in Bangladesh.
Study Design: Cross-sectional study using a semi-structured questionnaire.
Method: Primary data were collected by conducting an online survey with a semi-structured questionnaire. Data collection was carried out from March 2021 to October 2021. The subjects’ age range was 13–35. A total of 366 female students participated in the survey from different demographic profiles.
Results: 74.86% of respondents were between the ages of 21 and 25, and they were mostly undergraduate students (71.31%). 77.05% of respondents were familiar with the term PMS. PMS symptoms were experienced by almost all participants (94%) to different extents. 140 participants (38%) experienced PMS one week before their period. On the other hand, 152 participants (42%) were moderately affected by PMS physical symptoms. 43% of participants rated PMS psychological and behavioral symptoms as moderately severe. The most common PMS symptom, according to 259 female students, was cramping, followed by headache and backache. PMS causes 65.85% of participants to lose concentration during educational activities. 59.56% of the participants claimed PMS causes difficulty at work and in other regular activities.
Conclusion: PMS is highly prevalent among female students in Bangladesh. The majority of students experience a lack of concentration on educational activities due to PMS. PMS has an impact on both their personal and professional lives. Personal hygiene, sexual health, and overall awareness about PMS should be promoted more through education and social awareness programs.
Keywords
premenstrual syndrome, PMS, regular life of students, reproductive health, educational activities, social life, low-middle income country, survey
Abbreviations
PMS: premenstrual syndrome; ACOG: American College of Obstetricians and Gynecologists; WHO: World Health Organization; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; PMDD: premenstrual dysphoric disorder
Introduction
Over the last century, premenstrual syndrome (PMS) has become a recognized medical condition. Initially, it was supposed to be an ‘imagined’ sickness that only existed in the minds of ‘crazy’ women. Later, it was assumed that the female reproductive organs had entire control over the woman and that diverting energy away from the reproductive organs resulted in inadequate performance. As a result, women who worked physical labor required more treatments than those who merely used their minds [1]. PMS is defined as a group of symptoms that are uncomfortable enough to interfere with everyday functioning in 20–40% of women [2]. According to the American College of Obstetricians and Gynecologists (ACOG), PMS is a clinical condition characterized by the cyclic presence of physical and emotional symptoms unassociated with any organic disease that arise during the five days before menstruation in each of the three previous menstrual cycles and disappear within four days of menstruation occurrence, with no recurrence until at least cycle day 13 [3]. As of 2010, the World Health Organization (WHO) estimated that 199 million women suffered from PMS [4]. Although the actual prevalence of PMS is unknown, it is estimated that 70–90% of menstrual women have symptoms prior to their period. According to epidemiological research, up to 75% of reproductive-age women have symptoms related to the premenstrual phase of the menstrual cycle. In one research of adolescent participants, 100 percent of the individuals experienced at least one mild premenstrual symptom [5]. Previous studies have found conflicting results regarding the effects of behavioral and physical symptoms of PMS on health-related quality of life [6].
Pathophysiology of PMS and influencing factors
PMS has yet to be definitively linked to a pathophysiological cause. Early theories suggested that there were alterations in ovarian sex steroid levels, but this has been invalidated since no changes in progesterone levels have been found between symptomatic and asymptomatic women [7, 8]. Several ideas have been offered, ranging from sex hormone interactions to central nervous system neurotransmitter interactions. Estrogen excess or withdrawal, progesterone shortage, vitamin B6 deficiency, altered glucose metabolism, and fluid-electrolyte imbalances are some of the older ideas that have been found to be inaccurate. PMS, according to sociocultural theory, is a consequence of a conflict between society’s expectations of a woman’s dual position as a productive member of the workforce and a mother. PMS may be a cultural manifestation of women’s discontent with their conventional positions in society, according to this theory [1]. Although the exact cause of PMS is unknown, it is assumed to be linked to hormonal changes that occur around ovulation, and several factors may be involved. However, previously conducted studies have elucidated that there may be some factors working behind PMS, which include hormonal changes, chemical changes in the brain, body weight, inadequate physical exercise, mental stress, diet, postpartum depression, and some other factors as well [9, 10].
Major symptoms of PMS and other associated health problems
PMS symptoms range from mild to severe, interfering with everyday personal and professional life. Physical, psychological, and behavioral symptoms are the three most prevalent types. Physical symptoms include cramping, weight gain, abdominal bloating, tender and lumpy breasts, swollen ankles, headaches, backaches, skin changes and acne, upset stomach, insomnia, tiredness, joint aches, and dizziness [9]. Common psychological symptoms are irritability and mood swings, loss of confidence, feeling anger, feeling upset and emotions, depressed mood, tearfulness, anxiety, poor concentration, and restlessness. Behavioral PMS symptoms include food cravings, overeating, and loss of interest in sexual activities along with other symptoms [9, 10].
In a woman experiencing premenstrual symptoms, there might be several patterns of actual or perceived comorbidity. For starters, she might get another psychological disease later in life (lifetime comorbidity). Second, she might be suffering from a long-term mental or general medical problem, as well as premenstrual symptoms that aren’t related to the co-occurring disorder (concurrent comorbidity). Third, she might be suffering from a psychological or general medical issue that worsens before her period, a condition known as premenstrual exacerbation [11]. Some studies showed that women who want PMS medication may also be suffering from another health issue, which may worsen in the weeks leading up to their menstrual period [12]. These health issues share many of the same symptoms as PMS, including depression and anxiety disorders, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and some other issues as well [13, 14]. Some women claim that just before their menstruation, their symptoms become more severe. PMS can also exacerbate some health issues, such as asthma, allergies, and migraines [15, 16].
The effects of PMS on women’s regular lives
PMS is a collection of affective, behavioral, and physical symptoms. These symptoms can impair productivity and quality of life for women. PMS can affect the social functioning, work productivity, education, healthcare use, and overall quality of life of women of reproductive age [17]. Menstrual-related depression has been identified as a major morbidity among female university students. 37.2% of university students are at a high or very high risk of developing a mental condition. According to the WHO, 20–31% of university students worldwide suffer from at least one mental condition related to menstrual difficulties. PMS is linked to reduced positive academic affect and lower frontal rest asymmetry scores, both of which are linked to reward processing dysfunction, lower productivity, and interference with studies [18]. PMS also has an impact on efficiency and productivity, such as homework, social activities, friendships or family relationships, and difficulty concentrating. Adolescents with PMS do worse in school than those who do not experience PMS. PMS can also impact an individual’s mental health and social life. Women suffering from PMS frequently miss work or school, resulting in a lower quality of life. This is related to factors such as premenstrual pain and a stressful environment [19]. However, the higher prevalence of PMS among university students enrolled in health-related courses, as well as its impact on their quality of life, point to the importance of implementing educational practices that inform women about the syndrome because once reported, women are more likely to seek treatment, reducing the incidence of the syndrome and its negative impact on quality of life [20]. The aim and objectives of this study are:
- To evaluate the symptoms of PMS among female students in Bangladesh.
- To assess the severity of PMS symptoms and their impact on students’ quality of life.
- To learn about the level of knowledge about PMS among female students.
- To identify female students’ awareness level in this regard and to give them some insights.
Materials and Methods
Type of study
This is a cross-sectional study designed to find out the prevalence and severity of PMS among female students in Bangladesh and their impact on students’ quality of life.
Study area
The survey for this study was conducted on female students from different institutions and organizations in Bangladesh. Women from other schools, colleges, and universities across the country participated in this study.
Sample characteristics
A semi-structured questionnaire was constructed based on the study’s objectives by following previous literature. Both quantitative and qualitative data were included. Since this survey is being done during the COVID-19 pandemic, people are more likely to engage in internet activities, making online data collection the most practical technique. Data was gathered between March 2021 and October 2021. A total of 366 respondents from a range of ages and educational backgrounds took part in the study.
Inclusion and exclusion criteria
Subjects must be from any educational institution in Bangladesh. The age should be a minimum of 13 years. The minimum age limit of 13 was chosen to align with the age range of students attending secondary school in Bangladesh, ensuring a homogeneous sample of female students facing the challenges of managing PMS symptoms while pursuing education. This decision takes into account factors such as school enrollment age in Bangladesh and the onset of puberty, ensuring that subjects are likely to have reached the stage of experiencing PMS symptoms. Also, they must have a minimum knowledge of digital technology and should be able to fill out the online questionnaire. The participant has their consent to use their opinions in the questionnaire. People who declined to take part in this particular survey were not included in the study. People who were not from any region of Bangladesh were avoided in order to maintain the uniformity of the data.
Questionnaire development
Both Bengali and English were used in the questionnaire’s construction. To prevent unwanted semantic confusion, they were written in plain language. Before creating the final forms, all the questions were thoroughly examined for their relevance to the research with the assistance of the research supervisor. Multiple-choice options were available for some specific questions. Extra space was provided after some questions for the participants’ comments; in most cases, these were used as qualifying remarks, which aided significantly in delivering responses to specific questions, such as participants mentioned if they had experienced other PMS symptoms in addition to the given symptoms.
Sampling technique and data collection method
The stratified random sampling strategy was used in this study. Only female students represented the sample. For the survey, participants were chosen from a variety of age groups, educational backgrounds, socioeconomic classes, and ethnicities. Data were collected online using Google Forms via social networking sites and face-to-face interviews. The questionnaire form was spread through various open online platforms and groups, and responses were taken from those who willingly wanted to participate and fill out the questionnaire form. The authors used their social media networks, which included sites like Facebook, Messenger, and WhatsApp. After that, those responses were studied and assorted into different groups according to the respondent’s location or district. The population was split into groups, which are basically the districts of Bangladesh. The overall sample consists of random people from those districts. For participants who lacked email addresses, internet access, or a firm grasp of technology, some replies were also gathered via phone calls or in-person interviews. The questions were well-structured, and the respondents may either complete the form or react verbally.
Data analysis
After data gathering, Microsoft Excel 2016 was used to examine and evaluate them. Charts, tables, pie charts, and column diagrams were used to show the findings. In this study, only fundamental descriptive statistical values (percentages, frequency numbers, etc.) were determined rather than finding more diverse and complex correlation analysis test results. One of the basic aims of this study was to acquire a primary picture of the prevalence and impact of PMS among Bangladeshi students countrywide. The numbers and percentages of the final results sufficiently provided a basic and rudimentary idea about it; therefore, more complex statistical processes were avoided. Maybe these sorts of more diverse analytical values and tests can be used in future studies regarding this topic to show more sophisticated and impactful findings regarding the impact of PMS. Conclusions concerning the prevalence of PMS and its effects on students’ daily lives in Bangladesh were drawn after thoroughly analyzing the data.
Results and Discussion
PMS is a common health issue in women of reproductive age. It can significantly impact regular life activities, education, and the respective work performances of female students. In this study, it was tried to find out what kinds of physical, psychological, and behavioral symptoms people experience during PMS and the degree of those symptoms. Also, the impacts of PMS on educational activities, social activities, and interpersonal relationships were evaluated by analyzing the primary data that were collected by conducting a survey using a well-prepared questionnaire. This study included 366 female students of different age groups. They completed the questionnaire in the first part. Following the collection of primary data, the data were thoroughly checked and analyzed in the next phase. These data were analyzed by creating corresponding charts, tables, and diagrams for ease of use. The following results were obtained and evaluated after the data were thoroughly checked, analyzed, and studied. Percentages obtained throughout the analysis of the tables and figures were rounded up in some of the discussion parts for more convenience.
Firstly, the demographic conditions of the participants were evaluated in the below table (Table 1). In a survey of 15 to 49-year-old women, PMS was found to be highly prevalent in Pakistan and Turkey. While there has been little published research on PMS from Iran, it appears that PMS is prevalent in young girls there [4]. Here in our study, most of the respondents (274 participants) were from the age group 19–24 years, which is 75% of the total study population. Another demographic aspect is the educational status of the participants. 261 (71%) out of the 366 participants were ongoing undergraduates, which was the majority. Moreover, all of the study population were educated females.
| Elements | Sample number (n) | Percentage (%) |
| Total | 366 | 100 |
| Age group |
| 13–18 | 25 | 6.83 |
| 19–24 | 274 | 74.86 |
| 25–30 | 43 | 11.75 |
| 31–35 | 23 | 6.28 |
| 35+ | 1 | 0.27 |
| Educational status |
| PSC/JSC | 7 | 1.91 |
| Secondary | 15 | 4.10 |
| Higher-secondary | 23 | 6.28 |
| Under-graduate | 261 | 71.31 |
| Graduate | 55 | 15.03 |
| Others | 5 | 1.37 |
Table 1: Demographic characteristics.
Information and data regarding PMS and menstruation are demonstrated in the table (Table 2). For most of the subjects (32.24%), the first age of menstruation or ‘menarche’ was 12. About 25.14% attained menarche before 12. This study found no correlation between the age of menarche and the days of menstrual flow. Previous studies have identified either a positive or no correlation between the onset of menarche and blood flow during menstruation [21]. Almost 80% of them have normal blood flow during menstruation (between 3–8 days), and nearly 74% of them have a regular menstrual cycle length, which is 21–35 days, which indicates that the prevalence of polymenorrhea and oligomenorrhea is less among these students. In contrast, from the given table (Table 2), 32 participants have polymenorrhea, which means their menstrual cycle length is less than 21 days, and only 3% of participants have oligomenorrhea (menstrual cycle length of more than 90 days). According to a study, college students had limited knowledge about premenstrual disorder since the majority of students with PMS and premenstrual dysphoric disorder (PMDD) did not consider their symptoms to be abnormal [21]. However, 77% of this study population, which is way more than half, claimed that they were aware of the term ‘premenstrual syndrome (PMS)’ before the study, indicating a high level of awareness among the educated female participants. 38% of participants faced PMS one week before their period. A research article about premenstrual syndrome and its prevalence, severity, and impact on the daily life of students demonstrated that fewer than half of the students suffer from mild PMS physical symptoms [22]. Furthermore, around one-third of them exhibited mild PMS psychological and behavioral symptoms. More than one-third of the research participants experienced mild overall PMS symptoms, whereas more than a quarter had moderate PMS symptoms. Only 5.8% of them suffer from severe PMS symptoms. Our present study has shown a similarity with that. We can see from our study that 42% of the participants felt the physical symptoms of PMS moderately. On the other hand, psychological and behavioral symptoms were felt moderately by 43% of participants.
| Elements | Sample number (n) | Percentage (%) |
| Total | 366 | 100 |
| Age of first menstruation/period (menarche) |
| < 9 years | 5 | 1.37 |
| 9 years | 6 | 1.64 |
| 10 years | 18 | 4.92 |
| 11 years | 63 | 17.21 |
| 12 years | 118 | 32.24 |
| 13 years | 85 | 23.22 |
| 14 years | 48 | 13.11 |
| 15 years | 19 | 5.19 |
| > 15 years | 4 | 1.09 |
| Duration of your menstrual bleeding |
| 1–2 days | 12 | 3.28 |
| 3–4 days | 134 | 36.61 |
| 5–6 days | 158 | 43.17 |
| 7–8 days | 48 | 13.11 |
| > 8 days | 14 | 3.83 |
| Menstrual cycle length |
| 21–35 days | 270 | 73.77 |
| 35–90 days | 51 | 13.93 |
| < 21 days | 32 | 8.74 |
| > 90 days | 13 | 3.55 |
| Being aware of the term ‘premenstrual syndrome (PMS)’ |
| Yes | 282 | 77.05 |
| No | 31 | 8.47 |
| Maybe | 53 | 14.48 |
| How long before period do PMS start |
| 1 week before period | 140 | 38.25 |
| 2 weeks before period | 32 | 8.74 |
| 4–5 days before period | 119 | 32.51 |
| 2–3 days before period | 65 | 17.76 |
| Other | 10 | 2.73 |
| Degree of feeling the physical symptoms of PMS |
| Mild | 129 | 35.25 |
| Moderate | 152 | 41.53 |
| Severe | 63 | 17.21 |
| No | 22 | 6.01 |
| Degree of feeling the psychological and behavioral symptoms of PMS |
| Mild | 97 | 26.50 |
| Moderate | 159 | 43.44 |
| Severe | 86 | 23.50 |
| No | 24 | 6.56 |
| PMS physical symptoms |
| Swollen or tender breasts | 96 | 26.23 |
| Headache or backache | 219 | 59.84 |
| Constipation or diarrhea | 81 | 22.13 |
| Bloating or a gassy feeling | 124 | 33.88 |
| Cramping | 259 | 70.77 |
| Pimples/acne | 193 | 52.73 |
| Hunger | 124 | 33.88 |
| Other | 16 | 4.37 |
| PMS psychological and behavioral symptoms |
| Feeling tired | 259 | 70.77 |
| Sleep problems (sleeping too much or too little) | 203 | 55.46 |
| Trouble with concentration or memory | 156 | 42.62 |
| Irritability or hostile behavior | 189 | 51.64 |
| Depression, feelings of sadness, or crying spells | 228 | 62.30 |
| Mood swings | 293 | 80.05 |
| Tension or anxiety | 185 | 50.55 |
| Angry outbursts | 208 | 56.83 |
| Others | 1 | 0.27 |
| PMS is making several other health issues worse |
| Yes | 109 | 29.78 |
| No | 156 | 42.62 |
| Maybe | 101 | 27.60 |
| Health problems that worsen due to PMS |
| Asthma | 22 | 6.011 |
| Allergies | 53 | 14.481 |
| Migraine | 108 | 29.508 |
| Not prefer to answer | 213 | 58.197 |
| Other | 14 | 3.825 |
| Home remedy/treatment during PMS |
| Avoid rich food | 92 | 25.14 |
| Avoid excessive salt, caffeine, and alcohol | 104 | 28.42 |
| Exercise | 78 | 21.31 |
| Get enough sleep | 248 | 67.76 |
| Track your moods and symptoms in a journal | 55 | 15.03 |
| Others | 21 | 5.74 |
| Medicines that have been taken during PMS |
| Pain killer | 196 | 53.55 |
| Medicine for acidity/gastric | 100 | 27.32 |
| Anti-vomiting | 17 | 4.64 |
| Anti-depressant | 24 | 6.56 |
| Vitamin, mineral or other supplements | 73 | 19.95 |
| Birth control or oral contraceptive pills | 7 | 1.91 |
| Others | 17 | 4.64 |
| From whom help is gotten most of the time during PMS |
| Mother | 223 | 60.93 |
| Friends | 101 | 27.60 |
| Teacher | 3 | 0.82 |
| Siblings | 77 | 21.04 |
| Other family members | 33 | 9.02 |
| None | 92 | 25.14 |
| Others | 5 | 1.37 |
| Knowledge about the impact of food in menstruation |
| Yes | 162 | 44.26 |
| No | 145 | 39.62 |
| Maybe | 59 | 16.12 |
| Visiting doctor, clinician or any hospital for the PMS problem |
| Yes | 99 | 27.05 |
| No | 267 | 72.95 |
| Participation in social awareness activity regarding premenstrual syndrome (PMS) |
| Yes | 41 | 11.20 |
| No | 95 | 25.96 |
| Have seen but never taken part | 46 | 12.57 |
Table 2: Data and information regarding menstruation and PMS.
A study showed that, in PMS patients, the most common physical symptom was abdominal bloating, which was experienced by 89.5% of the students, while the most common emotional symptom was irritation (88.3%). According to Goker et al. [23], breast tenderness was the most common physical issue, affecting 35.5% of Nigerian university students. In a survey of Lebanese medical students, breast tenderness was the most common symptom, with a rate of 65%, followed by abdominal bloating and headache [23]. However, in this present study, we can see from the figure (Figure 1) that the most frequent physical symptoms were cramping (259 responses), and the second most chosen symptoms were headache or backache; 219 people chose it. Also, mood swings (293) were the most frequent psychological and behavioral symptoms, according to the data from the figure (Figure 2). According to research, PMS was found to be substantially correlated with a variety of educational issues, including lack of concentration, lack of ambition, poor individual or group task performance, and low test scores [3]. Another study showed that, among university students, mood states (dysphoria) showed a substantial negative connection with academic achievement. As a result, their academic performance is more likely to decline [24]. A study about “The effect of PMS symptoms on daily life activities in Korean women” stated that the more severe the woman’s PMS symptoms were, the more unfavorable her influence on everyday life activities was. Furthermore, somatic symptoms had the most significant influence on basic life activities [25]. Similarly, we can see in this study that 241 respondents (65.85%), which means more than half of the students face a lack of concentration on educational activities due to PMS. As the majority of the participants faced a lack of concentration on education, their academic performance was also affected. 140 of them claimed that their academic performance was affected mildly due to PMS. More than half of the population (59.56%) claimed that they face difficulties in working and other activities due to PMS. Their relationship with others (30.87%) and their social activities (31.42%) were affected mildly. More than one-third of the population claimed that PMS does not make several health issues worse, while some participants thought that it does make them worse (101 participants), and the rest of them (109 participants) were unsure about it, and these two numbers were quite close. Here, migraine was the most common (108 responses) health issue, while there were some other issues pointed out by them, such as asthma (22 responses), allergies (53 responses), etc., that also got worse. However, a majority of participants preferred not to answer this question.
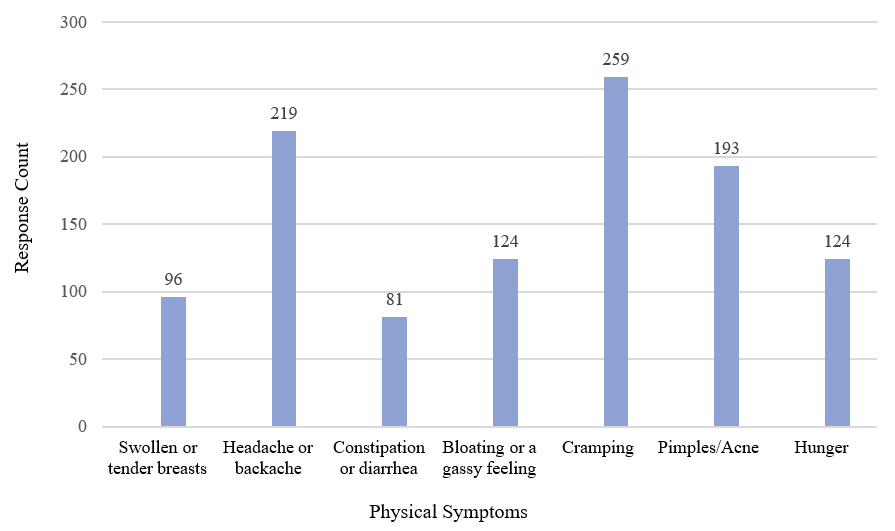 Figure 1: Distribution of total participants according to their PMS physical symptoms.
Figure 1: Distribution of total participants according to their PMS physical symptoms.
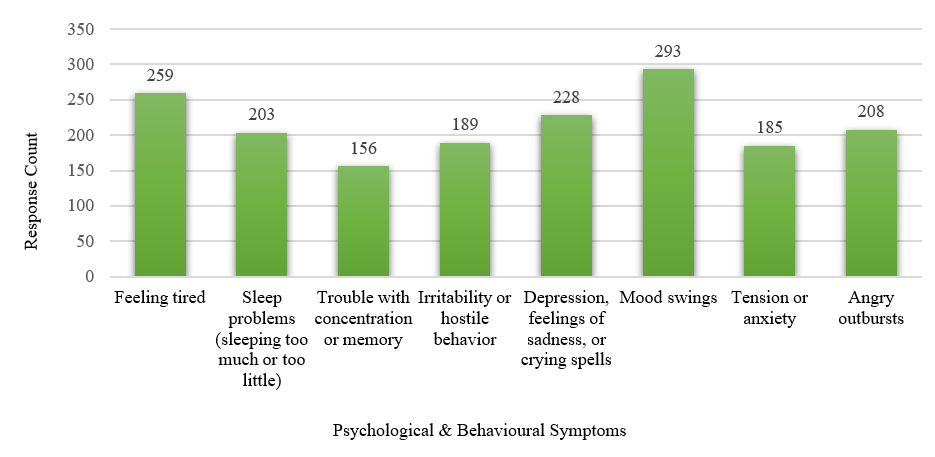 Figure 2: Distribution of total participants according to their PMS psychological and behavioral symptoms.
Figure 2: Distribution of total participants according to their PMS psychological and behavioral symptoms.
To alleviate PMS symptoms, several home remedies/treatments were taken by the participants, which are shown in the table (Table 2). The majority of them (248 participants) got adequate sleep. 104 participants avoided rich foods, caffeine, and alcohol during PMS. To treat PMS symptoms, painkillers were taken by 196 respondents to treat cramping, headache, and backache. Some other drugs like medicine for acidity/gastric (100 participants), vitamins, minerals, or other supplements (73 participants), anti-vomiting (17 participants), anti-depressants (24 participants), etc. were also taken by them during PMS, according to the given figure (Figure 3). The majority of the participants (223 participants) sought help from their mothers during PMS. 44% of students had an idea about how their food habits can impact their menstrual health, while almost a similar number of participants (40%) didn’t have any idea about that. Many studies showed that foods like dairy products, caffeine, rich foods, etc., can worsen the symptoms of PMS. That is why we saw that 104 participants avoided these kinds of foods during PMS. The table (Table 2) found that more than half of the participants, 73% (267 participants), had never visited a doctor, clinician, or any hospital for the PMS problem. However, we have found that they take several kinds of medicines. Therefore, it can be self-medication, which is quite highly prevalent in Bangladesh, according to a recent study [26]. So, there is definitely some unawareness present among the majority of these people. Most of them (52%) said that they had never participated in or seen any social awareness program like seminars, discussions, or even any online activity about PMS.
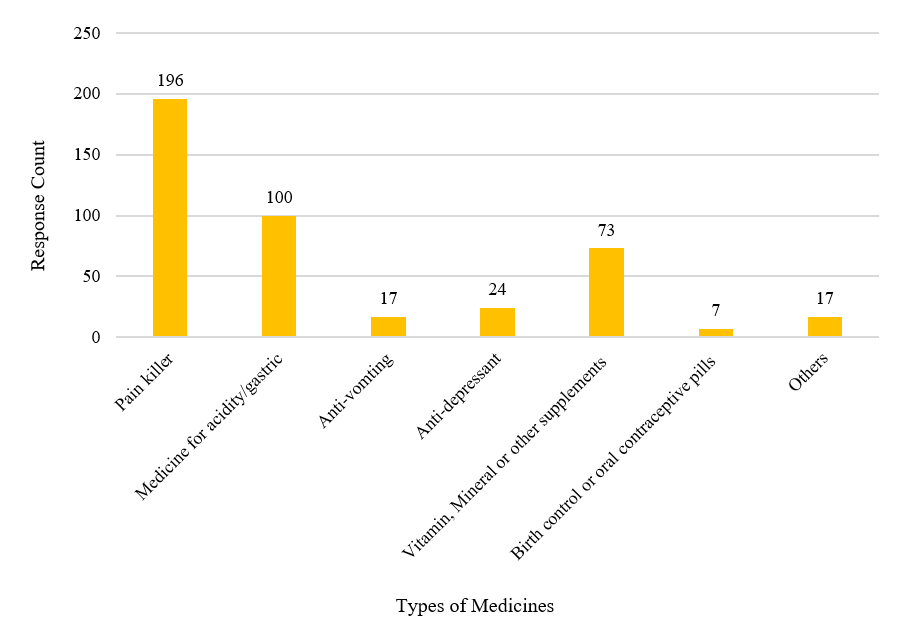 Figure 3: Distribution of total participants according to medicines that have been taken during PMS.
Figure 3: Distribution of total participants according to medicines that have been taken during PMS.
The impact of PMS on education and the regular lives of students is detailed in the table below (Table 3). From the above-mentioned table, we can see that students were asked if they faced a lack of concentration on ‘educational activities’ due to PMS. Among 366 respondents, 241 students (65.85%) reported a lack of concentration on their education due to PMS. Only 44 students (12.02%) stated that they did not face a lack of concentration due to PMS. On the other hand, 81 students (22.13%) were not sure if they faced a lack of concentration on educational activities due to PMS. A study which was done in Jordan demonstrated that PMS and premenstrual dysphoric disorder (PMDD) symptoms have a severe impact on the academic performance of female students [24]. In our study, the students were asked if PMS had any effect on their ‘academic performance.’ Out of 366 respondents, 140 respondents (38.25%) reported that they had ‘mild’ PMS effects on their academic performance. Consequently, 113 (30.87%) students responded that they had ‘moderate’ effects of PMS on their academic performance. Only 38 students (10.38%) had a severe impact, and 75 students (20.49%) reported that PMS did not interfere with their academic performance. According to the findings of a study conducted at Foundation University Medical College, Islamabad, PMS was identified in the majority of the students, and the majority of students agreed that it had an impact on academic achievement [27]. Next, we can see in the table (Table 3) that the participants were asked if they had faced any difficulties working on other activities due to PMS. A majority of the participants, 218, answered affirmatively (59.56%). 81 participants (22.13%) did not face any difficulties in working and other activities due to PMS, and 67 participants (18.31%) were not sure if they encountered any problems due to PMS. A previous study also showed that the impact of PMS symptoms on women’s workdays and their productivity is a serious problem [28]. According to the table (Table 3), the students were then asked about the effects of PMS on relationships with others. 113 participants (30.87%) out of 366 reported that PMS mildly affects their relationships with others. Then, 97 participants (26.50%) stated that they had moderate effects, 51 participants reported severe effects, and 105 participants (28.69%) reported having no impact of PMS on their relationships with others. Another relevant study showed that PMS symptoms had a negative effect on female students’ academic performance and mental well-being, and there was also a significant reduction in work productivity and social life functioning [29]. Furthermore, in the table (Table 3), we can see that students were asked if they had faced any effects of PMS on their social activities. Only 103 participants (28%) reported no impact on their social activities due to PMS. While 115 participants (31.42%) reported mild, 106 participants (28.96%) reported moderate, and 42 participants (11.48%) reported severe effects of PMS on their social life activities.
| Elements | Sample number (n) | Percentage (%) |
| Lack of concentration on educational activities |
| Yes | 241 | 65.85 |
| No | 44 | 12.02 |
| Maybe | 81 | 22.13 |
| Effects of PMS on academic performance |
| Mild | 140 | 38.25 |
| Moderate | 113 | 30.87 |
| Severe | 38 | 10.38 |
| No | 75 | 20.49 |
| Difficulties in working and other activities due to PMS |
| Yes | 218 | 59.56 |
| No | 81 | 22.13 |
| Maybe | 67 | 18.31 |
| Effects of PMS on relationship with others |
| Mild | 113 | 30.87 |
| Moderate | 97 | 26.50 |
| Severe | 51 | 13.93 |
| No | 105 | 28.69 |
| Effects of PMS on social activities |
| Mild | 115 | 31.42 |
| Moderate | 106 | 28.96 |
| Severe | 42 | 11.48 |
| No | 103 | 28.14 |
Table 3: Association of PMS on educational activities and regular life of students.
However, this study also has some limitations, which put forward some questions for future researchers in this field. As we have seen here, the majority of our participants (73%) had never visited a doctor, clinician, or any hospital for the PMS problem. However, we have found that they take several kinds of medicines. Therefore, it can be self-medication practice which is highly prevalent in Bangladesh [26], and more rigorous studies are needed to asses it’s limits, benefits, and risks in terms of PMS. In addition to that, since the participants self-reported their symptoms and information via the questionnaire, we cannot completely ensure we gathered all the relevant data without any erroneous response. Although it is challenging to remove it in questionnaire-based studies, this kind of bias can affect some of the findings. The findings of this study are limited in their generalizability due to the small sample size and short time frame. To further understand this issue, future research should focus on both urban and rural areas and include patients as much as feasible.
Conclusion
PMS is highly prevalent among female students in Bangladesh. PMS, in its most severe form, has a negative impact on a female student’s social and academic performance. According to our research, physical, psychological, and behavioral symptoms were primarily experienced in moderate amounts. However, we can tell from this study that cramping was the most common physical complaint, and headache or backache was the second most common symptom. Mood swings were also the most common psychological and behavioral symptom. In this study, we can see that more than half of the students have difficulty concentrating on educational activities due to PMS. Because the majority of the participants were unable to focus on their studies, their academic performance suffered as a result. PMS causes difficulty in working and other activities for the majority of the population. Their social activities and relationships with others were both mildly affected. This study provides information about PMS and its impact on students’ quality of life, allowing for more informed advice on the subject. Healthcare professionals can help women recognize and manage these frequent disorders by educating them about premenstrual symptoms and counseling them on lifestyle changes and medication to alleviate their symptoms. The syndrome and its prevention should be promoted through education and social awareness programs.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Department of Pharmacy, East West University. Survey participants were informed that the information collected would be kept anonymous and that their role in the study would be entirely voluntary.
Author Contributions
All authors contributed equally to this work.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Availability of Data and Materials
All datasets generated or analyzed during this study are included in this article.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgments
The authors would like to express their sincere thanks to all the participants. They also express their gratefulness to the Chairperson of the Department of Pharmacy, East West University, Dr. Sufia Islam. Furthermore, they express their sincerest appreciation to all the teachers and staff in the Department of Pharmacy, East West University.
References
- Fiebai P, Ukueku AO, Ogu R. Pre Menstrual Syndrome. In: Lutsenko OI. Menstrual Cycle. IntechOpen; 2018.
- Braverman PK. Premenstrual syndrome and premenstrual dysphoric disorder. J Pediatr Adolesc Gynecol. 2007;20(1):3-12.
- Buddhabunyakan N, Kaewrudee S, Chongsomchai C, et al. Premenstrual syndrome (PMS) among high school students. Int J Womens Health. 2017;9:501-05.
- Farrokh-Eslamlou H, Oshnouei S, Heshmatian B, et al. Premenstrual syndrome and quality of life in Iranian medical students. Sex Reprod Healthc. 2015;6(1):23-7.
- Zaka M, Mahmood KT. Pre-menstrual syndrome- A review. J Pharm Sci Res. 2012;4(1):1684-691.
- Rapkin AJ, Winer SA. Premenstrual syndrome and premenstrual dysphoric disorder: quality of life and burden of illness. Expert Rev Pharmacoecon Outcomes Res. 2009;9(2):157-70.
- Walsh S, Ismaili E, Naheed B, et al. Diagnosis, pathophysiology and management of premenstrual syndrome. Obstet Gynaecol. 2015;17(2):99-104.
- Hickey M, Balen A. Menstrual disorders in adolescence: investigation and management. Hum Reprod Update. 2003;9(5):493-504.
- Women’s Health Concern. Premenstrual Syndrome (PMS). 2012.
- Mishra A, Banwari G, Yadav P. Premenstrual dysphoric disorder in medical students residing in hostel and its association with lifestyle factors. Ind Psychiatry J. 2015;24(2):150-57.
- Yonkers KA, O’Brien PM, Eriksson E. Premenstrual syndrome. Lancet. 2008;371(9619):1200-210.
- Lawrence H. The American college of obstetricians and gynecologists supports access to women’s health care. Obstet Gynecol. 2015;125(6):1282–284.
- Bailey JW, Cohen LS. Prevalence of mood and anxiety disorders in women who seek treatment for premenstrual syndrome. J Womens Health Gend Based Med. 1999;8(9):1181-184.
- Padhy SK, Sarkar S, Beherre PB, et el. Relationship of premenstrual syndrome and premenstrual dysphoric disorder with major depression: relevance to clinical practice. Indian J Psychol Med. 2015;37(2):159-64.
- Woods NF, Most A, Dery GK. Prevalene of perimenstrual symptoms. Am J Public Health. 1982;72(11):1257-164.
- Rizk DE, Mosallam M, Alyan S, et al. Prevalence and impact of premenstrual syndrome in adolescent schoolgirls in the United Arab Emirates. Acta Obstet Gynecol Scand. 2006;85(5):589-98.
- Kumari S, Sachdeva A. Patterns and Predictors of Premenstrual Symptoms among Females Working in a Psychiatry Hospital. Scientifica (Cairo). 2016;2016:6943852.
- Al-Shahrani AM, Miskeen E, Shroff F, et al. Premenstrual Syndrome and Its Impact on the Quality of Life of Female Medical Students at Bisha University, Saudi Arabia. J Multidiscip Healthc. 2021; 14:2373-379.
- Kustriyanti D, Rahayu H. Prevalence of premenstrual syndrome and quality of life among health science college student. Int J Public Heal Sci. 2020;9(1):15–9.
- Victor FF, Souza AI, Barreiros CDT, et al. Quality of Life among University Students with Premenstrual Syndrome. Rev Bras Ginecol Obstet. 2019;41(5):312-17.
- Durairaj A, Ramamurthi R. Prevalence, pattern and predictors of premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) among college girls. New Indian J OBGYN. 2019;5(2):93-98.
- Elgzar WTI. Premenstrual Syndrome: Prevalence, Severity and Impact on Daily Life Activates among Medical Students at Najran University KSA. Indo Am J Pharm Sci. 2019;6(9):12104-2112.
- Goker A, Artunc-Ulkumen B, Aktenk F, et al. Premenstrual syndrome in Turkish medical students and their quality of life. J Obstet Gynaecol. 2015;35(3):275-78.
- Hussein Shehadeh J, Hamdan-Mansour AM. Prevalence and association of premenstrual syndrome and premenstrual dysphoric disorder with academic performance among female university students. Perspect Psychiatr Care. 2018;54(2):176-84.
- Choi D, Lee DY, Lehert P, et al. The impact of premenstrual symptoms on activities of daily life in Korean women. J Psychosom Obstet Gynaecol. 2010;31(1):10-15.
- Jami MABS, Biswas K. A cross-sectional study regarding the knowledge, attitude and awareness about self-medication among Bangladeshi people. Heal Policy Technol. 2023;In Press:100715.
- Kalsoom DU, Sultana A, Amjad T, et al. Prevalance of premenstrual syndrome and knowledge assessment regarding it’s prevention among medical students of a private medical college of Islamabad. Pakistan Armed Forces Med J. 2018;68(1):159-64.
- Hylan TR, Sundell K, Judge R. The impact of premenstrual symptomatology on functioning and treatment-seeking behavior: experience from the United States, United Kingdom, and France. J Womens Health Gend Based Med. 1999;8(8):1043-052.
- Nisar N, Zehra N, Haider G, et al. Frequency, intensity and impact of premenstrual syndrome in medical students. J Coll Physicians Surg Pak. 2008;18(8):481-84.
