Background: Menstrual disorders affect women all around the world, although they are still viewed as minor health problems.
Objective: The objective of this study is to investigate the prevalence of menstrual disorders among modern society females in Dhaka, Bangladesh, and explore potential factors that may influence these disorders.
Study Design: It is a cross-sectional study using a convenient sampling technique.
Method: A convenient sampling technique was used to collect primary data through a semi-structured questionnaire from 342 female residents of Dhaka, aged at least 15 years, between April 2021 and August 2021. Participants were from different demographic backgrounds.
Results: The mean age of respondents was 22 years ± 8.03. Participants were predominantly educated, with many pursuing undergraduate studies. They mostly belonged to nuclear families (77.7%) and middle (59.5%) to upper-middle (33.1%) socio-economic classes. Prevalent premenstrual symptoms included a change in mood (71.6%), cramps (68.9%), abdominal bloating (45.9%), and breast discomfort (38.5%). Dysmenorrhea (50.6%) and menorrhagia (35.2%) were common, while polymenorrhea (10.8%) and oligomenorrhea were less frequent. Despite some knowledge about the negative influence of junk foods on menstrual health, a significant proportion of participants reported consuming junk foods regularly. Most participants had easy access to sanitary napkins and menstrual hygiene products.
Conclusion: Menstrual disorders are prevalent among young women in modern Dhaka despite their good education rate. Lifestyle and diet are linked to their prevalence. Healthcare professionals must educate and counsel women on menstrual health. Collaborative efforts among professionals, policymakers, and researchers are needed to raise awareness and support women in managing these issues.
Menstruation is a natural phenomenon characterized by the outflow of blood from the uterine wall through the vagina approximately at regular monthly intervals during female reproductive life [1]. One of the most common gynecologic problems in reproductive health is menstrual disturbances. While some women experience only mild discomfort or anxiety during their monthly periods, others go through severe physical and emotional symptoms, including heavy bleeding, missed periods, mood swings, and painful menstruation, which affect a woman’s quality of life [2]. Menstrual disorders can begin as early as menarche and can last well into adolescence when additional stressors such as life challenges, academics, and relationships aggravate the symptoms [3]. According to studies, women of reproductive age have health issues related to their periods. Menstrual problems can take many different forms, including dysmenorrhea, oligomenorrhea, premenstrual syndrome (PMS), and polymenorrhea. Menorrhagia, amenorrhea, and irregular menstruation are all symptoms of abnormal vaginal bleeding [4].
There are many various types of menstrual disorders. Heavy, excruciating periods or no periods at all can be problems [5]. Although there are many variations in the length of their cycles, generally speaking, women should be worried if their cycles are less than 21 days long, more than 3 months apart, or more than 10 days long. Such occurrences might point to menstruation issues or other illnesses. Menstrual cramps that are intense and persistent are known as dysmenorrhea. Although it usually starts in the lower abdomen, pain can also travel through one’s lower back and legs. Usually, dysmenorrhea is classified as primary or secondary [6]. Menstrual discharge that lasts longer and is heavier than usual is known as menorrhagia, and the bleeding happens daily (during periods). It typically lasts longer than 7 days, and women lose excessive quantities of blood (more than 80 mL). Dysmenorrhea frequently occurs alongside menorrhagia because large clots can cause excruciating cramping while moving them [5]. Menstruation is absent in amenorrhea. Primary amenorrhea and secondary amenorrhea are the two types. Menstrual cycles are light or infrequent and spaced out by more than 35 days in oligomenorrhea, a menstrual disorder. It is very typical in early puberty and typically does not signify a health issue [2, 5]. PMS is a group of symptoms that, in the majority of periods, appear during the final week of the luteal phase (one week before menstruation). Usually, the symptoms don’t appear until at least day 13 of the period, and they go away four days after the bleeding starts. PMS signs can appear in women at any point throughout their reproductive years, but they typically do so between the ages of 20 and 40 [7, 8].
In addition to the pathological factors that interfere with women’s cycles, depression, smoking, changes in body weight, stress, and other environmental factors have been documented to affect the menstrual pattern [9]. Disturbances linked to menstruation may have a significant impact on students’ physical and psychological health. These issues can lead to adolescent problems and issues for their families during this challenging developmental period, which in turn contributes to school absences [6]. Menstrual problems are considered normal among women and a situation that does not necessitate medical attention. When the condition becomes unbearable, the few who seek medical assistance are forced to believe so and are not provided with proper medical help. Often, many choose to self-medicate themselves rather than go to doctors without having the proper knowledge and also without knowing the risks and benefits of self-medication. This issue is also quite prevalent in developing countries like Bangladesh [10]. Although many reasons have been advanced for the lack of attention paid to menstrual issues, some regard it as a “taboo” that should not be discussed in public, while others believe it is a private matter [3]. There aren’t many studies in the literature about how common menstrual issues are among women in Bangladesh who are of reproductive age. The majority of current studies lacked a clear socio-economic emphasis. The goal of this research is to investigate the prevalence of menstrual disorders and symptoms in Dhaka’s modern society so that this information can be used by policymakers and healthcare authorities to design targeted interventions and awareness campaigns to improve menstrual health education and access to proper healthcare services. It can also lead to the inclusion of menstrual health in reproductive health programs and policies. The objective of this study is to investigate the prevalence of menstrual disorders among modern society females in Dhaka, Bangladesh, and explore potential factors that may influence these disorders.
Survey design and participants
A cross‐sectional semi-structured questionnaire survey was conducted among Bangladeshi female citizens aged 15 years and older from April 2021 to August 2021. A convenience sampling strategy was used in this study, and a semi-structured questionnaire was developed to collect data. Data was collected primarily online using a Google form. The authors used their social media networks, which included sites like Facebook, Messenger, and WhatsApp, to circulate the questionnaire form and collect the data. Setting the minimum age at 15 years takes into account factors such as high school enrollment age in Bangladesh and the onset of puberty. By targeting females aged 15 years and above, the study aims to include participants who are likely to have experienced menarche and are in their reproductive age group. This ensures that the study can capture data from females actively experiencing menstrual cycles and related issues, making the research more relevant and focused on menstrual disorders. Additionally, this age range helps simplify data collection and ensures compliance with ethical considerations related to involving minors in research studies. Both quantitative and qualitative primary data were collected. Such as what kind of period cycle disorder someone is facing and how long her period cycle etc. Since this study was being conducted in the Covid-19 pandemic situation, people were more engaged with online activities, and so this seemed the most convenient method to collect data. A letter of permission describing the study’s goals with a link to the questionnaire was posted to the social media posts to get in touch with the online respondents. The respondents were given enough information about the goal of the study as well as the right to participate or not. A total of 342 females in the reproductive age group participated in the survey, accepting our request. Since Bangladesh is a low-middle income developing country, it does not have a very large modern population with modern facilities, education, and environment. Dhaka is the most modern metropolis of Bangladesh with an emerging young modern society. While a larger sample size may be ideal, a well-designed study with a smaller sample size can still provide valuable insights and generate hypotheses for future research.
Questionnaire design
The research objective was clearly defined, which was to investigate the prevalence of menstrual disorders and symptoms in Dhaka’s modern society. This objective guided the formulation of questions aligned with the study’s purpose. A pilot survey was conducted to test the comprehensibility and appropriateness of the questions. The questionnaire was aimed to collect information relevant to our study goal from each participant, including their socio-demographic characteristics, food habits, menstrual characteristics, menstrual disorders, hygiene, etc. The questionnaire was set after keeping in mind that these are educated, young, modern society females. Their information was taken after obtaining their consent and making sure that their privacy would be protected completely. The questionnaire was created with the goal of collecting the most accurate data possible, taking into account the views of the modern Bangladeshi female population. It was written in English. The questionnaire was constructed in simple language to prevent unnecessary semantic misunderstanding. Extra space was provided after some questions for the participants’ comments. In most cases, this space was used for qualifying remarks, which helped much in delivering answers to particular questions and providing further details that helped the surveyor draw conclusions. A clear explanation of the study’s goals and the participant’s right to participate or decline was provided at the beginning of the questionnaire. This ensured that participants were aware of the research purpose and their voluntary involvement.
Data analysis
The collected data were cleaned and modified for statistical analysis. Microsoft Excel 2016 software for Windows is used for data input entry and statistical analysis. Calculations were made for descriptive statistics such as percentages, means, and standard deviations. Tables and diagrams were used to show the findings. After carefully examining the data, conclusive percentages and figures about the prevalence of PMS and its impact on students’ daily lives were observed. Conclusions concerning the assessment of the prevalence of menstrual disorders were drawn after thoroughly analyzing the data.
Data were collected through a survey using a partially structured questionnaire. Initially, 1154 individuals were invited to participate, and 342 of them agreed and took part in the survey. In the first phase, these participants completed the questionnaire. A total of 342 women participated in the survey, as shown in the table (Table 1). Their mean age was 22 years ± 8.03. Most of the participants (n = 284, 83.1%) belonged to the age group 20–24 years. Approximately one-fourth of all participants had education up to Higher Secondary, and the majority (n = 166, 48.6%) were undergraduates. Maximum participants (n = 312, 91.2%) were unmarried, and only 8.8% were married. Most of them belonged to nuclear families (n = 266, 77.7%) and were from the middle class (n = 203, 59.5%) or upper-middle-class families (n = 113, 33.1%). From the table (Table 2), among all participants, 120 (81.1%) like to eat junk foods or fast foods, and most of them 99 (66.9%) eat junk foods sometimes. Roughly, the similar proportions had (n = 135, 39.5%) or had not (n = 107, 31.3%) proper idea about how food habits can impact menstrual health as well as 29.3% (n = 100) were unsure about how food habits can impact menstrual health. As is found in the table (Table 3), around 2% (34) of the population reached menarche at the age of 12, and the number is the same for the age of 13. Approximately 65% of the females attained menarche at the age of 12–14. About 13% attained menarche before 12 (starting from 9), and around 25% of females reached menarche after 14. The mean age of menarche in our population was 12.59 years ± 1.34. The duration of menstrual bleeding for the majority (n = 185, 54.1%) of the participants was 4–5 days. Only 2% claimed the duration of 9 days or more. The mean cycle length was found to be 28 days. Maximum participants (n = 245, 71.6%) had a normal menstrual cycle between 21–35 days. It was abnormal for 10.8% of participants with less than 21 days. Also, 2% of participants claimed their menstrual cycle length was more than 90 days. From the table (Table 3), the majority of the population (n = 266, 77.7%) experienced premenstrual symptoms. Premenstrual symptoms such as a change in mood (71.6%), leg pain/cramps (68.9%), abdominal bloating (45.9%), and breast discomfort (38.5%) were found mainly along with some other mild to moderate symptoms. Information about menstrual disorders and menstrual hygiene of the participants is shown in the table (Table 4). About 35.1% (52) of participants experienced heavy bleeding during periods regularly, and 35.1% (52) faced it sometimes. In contrast, 29.7% (102) of participants claimed they did not experience it. Findings also show that 50.6% (173) of women experienced severe pain during their period. On the other hand, 15.5% (53) of women did not experience severe pain during the period. The prevalence rate of these menstrual disorders among the participants is presented in the figure (Figure 1). It was found that 58.1% (86) had never visited a doctor, clinician, or hospital for a menstrual problem. The rest (n = 143, 49.1%) claimed they visited clinicians for this cause. Most of the participants (n = 243, 71%) could buy sanitary napkins without any difficulties, whereas 15.6% (53) of participants face problems sometimes, and 13.4% (46) said that they usually face difficulties while buying sanitary napkins.
The menstrual cycle is an inevitable part of a woman’s life and an important indication of normal sexual and reproductive health. Still, in Bangladesh, there is a culture of silence that surrounds this topic, which creates a barrier for women to access any right information and even in seeking any help. It is still perceived as a taboo topic to be discussed out loud in public [11]. This study was conducted to find out the prevalence of menstrual disorders in the modernized society of the capital, Dhaka. In the table (Table 1), the socio-demographic characteristics of the female participants were evaluated. The majority of the participants were between the ages of 20 and 24, which was almost 83.1% of the total population. All the participants were educated. A large number of them were young adults. Most of them had completed their graduation or were undergraduates. Therefore, respondents were mainly students who were studying mostly in universities, colleges, or schools in Dhaka, Bangladesh, and also, few of them were job-holders. A large number of the participants (n = 312, 91.2%) were unmarried. Most participants (n = 78, 77.7%) belong to nuclear families, as nuclear family structure predominates in urban areas [12]. Such results were found in a similar study conducted in India, where it was found that the proportion of nuclear family households has increased in urban areas [13]. A large number of the participants belong to middle-class families (59.5%), and the other half majority belong to upper-middle-class families (33.1%). So, it is safe to say that the majority of participants belong to economically solvent families, where menstrual products should be easily accessible to them. A previous study found that a higher wealth index was associated with higher use of sanitary napkins among adolescent girls [14].
| Characteristics | Frequency (n) | Percentage (%) |
| Age group (years) |
| 15–19 | 30 | 8.8 |
| 20–24 | 284 | 83.1 |
| 25–29 | 25 | 7.4 |
| 30–34 | 2 | 0.7 |
| Mean age = 22 years ± 8.03 |
| Educational status |
| Secondary | 14 | 4.1 |
| Higher secondary | 92 | 27.0 |
| Graduation | 166 | 48.6 |
| Post-graduation | 55 | 16.2 |
| Others | 14 | 4.1 |
| Marital status |
| Unmarried | 312 | 91.2 |
| Ever married | 30 | 8.8 |
| Family condition |
| Joint family | 76 | 22.3 |
| Nuclear family | 266 | 77.7 |
| Socio-economic class |
| Upper-class | 9 | 2.7 |
| Upper-middle-class | 113 | 33.1 |
| Middle-class | 203 | 59.5 |
| Lower-middle-class | 16 | 4.7 |
Table 1: Socio-demographic characteristics of the participants.
| Characteristics | Frequency (n) | Percentage (%) |
| Like to eat junk-foods, fast-foods, etc. |
| Yes | 277 | 81.1 |
| No | 18 | 5.4 |
| Maybe | 46 | 13.5 |
| Frequency of junk food consumption |
| Very frequently | 76 | 22.3 |
| Sometimes | 229 | 66.9 |
| Seldom | 37 | 10.8 |
| Have proper idea about food’s impact on menstrual health |
| Yes | 135 | 39.5 |
| No | 107 | 31.3 |
| Maybe | 100 | 29.3 |
Table 2: Food habits of the participants.
| Characteristics | Frequency (n) | Percentage (%) |
| Age at menarche |
| 9 | 7 | 2.1 |
| 10 | 12 | 3.4 |
| 11 | 50 | 14.5 |
| 12 | 95 | 27.8 |
| 13 | 93 | 27.1 |
| 14 | 60 | 17.6 |
| 15 | 16 | 4.8 |
| 16 | 9 | 2.8 |
| Total | 342 | 100.0 |
| Mean age of menarche = 12.594 years ± 1.34 |
| Menstrual bleeding duration |
| 1–2 days | 7 | 2.0 |
| 2–3 days | 65 | 18.9 |
| 4–5 days | 185 | 54.1 |
| 6–7 days | 65 | 18.9 |
| 7–8 days | 16 | 4.7 |
| 9 or more days | 5 | 1.4 |
| Mean duration = 4.64 days ± 1.37 |
| Menstrual cycle length (in days) |
| Less than 21 | 37 | 10.8 |
| 23–35 | 245 | 71.6 |
| 35–90 | 55 | 16.2 |
| More than 90 | 5 | 1.4 |
| Experience of premenstrual symptoms |
| Yes | 266 | 77.7 |
| No | 40 | 11.6 |
| Maybe | 37 | 10.8 |
| Premenstrual symptoms experienced |
| Nausea/vomiting | 60 | 17.6 |
| Headache | 100 | 29.1 |
| Change in mood | 245 | 71.6 |
| Leg pain/cramps | 236 | 68.9 |
| Abdominal bloating | 157 | 45.9 |
| Breast discomfort/heaviness | 132 | 38.5 |
| Others | 26 | 7.7 |
Table 3: Menstrual characteristics of the participants.
| Heavy bleeding (menorrhagia) |
| Yes | 120 | 35.2 |
| No | 102 | 29.7 |
| Sometimes | 120 | 35.2 |
| Severe pain (dysmenorrhea) |
| Yes | 173 | 50.7 |
| No | 53 | 15.5 |
| Sometimes | 116 | 33.8 |
| Visited doctor/clinician/hospital for menstrual problem |
| Yes | 199 | 58.1 |
| No | 143 | 41.9 |
| Have access to sanitary napkins without any difficulties |
| Yes | 243 | 71.0 |
| No | 46 | 13.4 |
| Seldom faces problems | 53 | 15.6 |
Table 4: Menstrual disorders and hygiene of the participants.
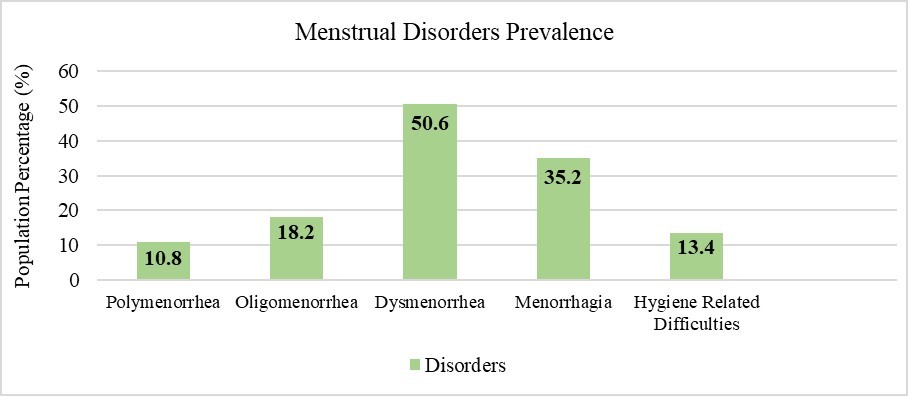 Figure 1: Prevalence of menstrual disorders among the participants.
Figure 1: Prevalence of menstrual disorders among the participants.
Moving to an important part of the discussion, the food habits of the female participants are shown in the table (Table 2). Upon being asked about their likings of junk food or fast food, most participants (n = 277, 81.1%) agreed to like eating junk food. Also, when asked about the frequency of consuming junk food, 66.9% (229) of them said they have it sometimes, and 22.3% said they consume it very frequently. Only a small number (n = 37, 10.8%) consume fast food seldom. These findings correlate to the findings of another study performed at Patuakhali Science and Technology University (PSTU), where 88.6% of that study agreed to eat junk foods very frequently [15]. From these responses, it is safe to say that young female adults in our modernized society are consuming fast foods very frequently, which can be a potential factor for many menstrual disorders, as a previous study has found [16]. A study performed among adolescent college girls in Kathmandu Valley shows that excessive consumption of junk food, tea-coffee, has a significant association with menstrual problems [17]. Then, the participants were also asked about their knowledge of the impact of food habits on their menstrual health. Among the participants, 135 (39.5%) agreed to know the impact of food habits on menstrual health well, and 31.3% (107) said they had at least some idea about it. Whereas 31.3% (107) of them had no idea how their food habits could influence their menstrual cycles and in a larger picture, their reproductive health. Junk food has adverse effects on health due to its low nutritional value, high levels of sugar, trans fats, and food additives. It can lead to many health issues, such as obesity, diabetes, heart disease, and skin cancers [18]. Literature also suggests that junk food consumption may be a risk factor for several menstrual disorders and polycystic ovary syndrome (PCOS) [19]. Most of the participants consuming junk foods even after having some knowledge about junk food’s negative influence on menstrual health is a sign of prevalent unawareness and improper education and also put forward the need for targeted interventions and educational programs to promote healthier dietary choices and menstrual health awareness among young women.
The table (Table 3) contains data related to the menstrual characteristics of the participants. The age of menarche is determined by genetics, socio-economic demography, general health, and nutritional factors [20]. In this study, 27.70 % and 27.02% of the study population were found to have encountered menarche at the ages of 12 and 13, respectively. Typically, menstrual flow lasts for 2–7 days. In our study, it was found that 185 (54.1%) respondents had an average flow consisting of 4–5 days, and 65 (18.9%) respondents had a bleeding period of 6–7 days, which is very normal for women of their age [21]. These findings are supported by the findings of the study performed at Dinajpur Medical College [22]. Normal variation of the menstrual cycle is 21–35 days with a mean of 28 ± 2 days. While it is considered irregular when less than 21 days or more than 35 days, the majority of the participants in the study have regular menstrual cycles since 245 respondents (71.6%) have a cycle consisting of 23–35 days, and this finding is also supported by some other studies [23, 24]. Premenstrual symptoms are the symptoms women experience in the weeks before the period. They can be caused by cyclic changes in the hormones, chemical changes in the brain (fluctuation of serotonin), or depression [25]. When asked about their experience of PMS, 77.7% (266) respondents among the 342 female participants admitted experiencing PMS, which ranges from feeling nauseated and vomiting to breast tenderness or heaviness and also several other symptoms that are presented in the table (Table 3). Among the PMS symptoms, change in mood was the most common, as 106 participants (n = 245, 71.6%) agreed to have them. Pain and cramps are another common PMS, having the second largest number of respondents (n = 236, 68.9%). Abdominal bloating (n = 157, 45.9%), breast discomfort (n = 132, 38.5%), and headache (n = 100, 29.1%) are also found to be significant PMS among our respondents, along with some other symptoms. Therefore, it was observed that the majority of participants suffered from several PMS symptoms. According to previous literature, menstrual headaches are a common kind of headache that affects women and are triggered by a decrease in estrogen levels during the menstrual cycle [26]. Gastrointestinal (GI) complaints are also common PMS symptoms among women [27]. In another study, one of the most common symptoms found among participants with PMS was breast tenderness and emotional outbursts [28]. However, according to a study by Alwafa et al. [29], common PMS symptoms include mood swings, depression, irritability, abdominal cramps, headache, generalized pains, abdominal bloating, swollen breast and tenderness, and appetite changes. The table (Table 4) sheds light on the topic of menstrual disorders and the hygiene patterns of the participants. A big portion of the respondents (n = 120, 35.2%) have said ‘yes’ to having heavy bleeding during their period, which is also known as menorrhagia, and another 35.2% have said that they face it sometimes, where only 29.7% (n = 102) said that they do not face this problem. According to a study, menorrhagia affects approximately 22% of healthy women worldwide [30]. However, in developing countries like Bangladesh, where adequate health-related awareness and education are not very available, and real-time studies evaluating these problems are also inadequate, the real prevalence rate can be more than the assumption. Dysmenorrhea is characterized by severe pain during periods. More than half of the participants, 50.6% (n = 173), have agreed to face severe pain during their period. Almost similar results were found in previous studies performed in PSTU (52.9%) and DMC (60.9%) [15, 22]. Prevalence percentages of these menstrual disorders among the participants of our study are shown in the figure (Figure 1). A higher level of education is associated with greater awareness and better knowledge about menstrual health. The findings of the study showed that most of the participants were educated young adults, which can be linked to their response to the question about visiting any clinician regarding their menstrual problems. Here, 199 participants (58.1%) have agreed to visit doctors for any kind of menstrual problems. Apart from this, most of the population belongs to solvent families, which should make sanitary napkins easily purchasable to them. This also supports our finding to the question where the participants were asked if they had easy access to sanitary napkins. To this question, a large number of participants (n = 243, 71%) have said that they have access to sanitary napkins without any difficulties. These findings are similar to the results obtained in a study performed previously in Bangladesh [31].
This study addresses a significant knowledge gap by shedding light on the prevalence of menstrual disorders in a modern society setting in Dhaka, Bangladesh. The information collected can serve as a foundation for further research and exploration of the factors contributing to menstrual disorders, such as lifestyle habits, stress, and access to menstrual hygiene products. The findings can inspire researchers to conduct larger-scale studies, use more advanced statistical methods, and investigate other potential risk factors and their interplay with menstrual health. However, the study does have some limitations. The study used convenience sampling and has a small sample size, as a result, the sample may not be generalized to the entire population of Bangladeshi women aged 15 years and older. Participants may not always provide accurate information in self-reported surveys, which may produce some bias. Future studies may consider using other data collection methods, such as direct observation or medical records. The study is limited in its ability to establish causal relationships between menstrual disorders and lifestyle factors due to its cross-sectional nature. Future research could employ longitudinal designs to better understand the cause-effect relationships between lifestyle choices, menstrual health, and the development of menstrual disorders. The data were only analyzed using descriptive statistics, which may not provide a comprehensive analysis of the data. Future researchers may consider using more advanced statistical techniques, such as regression analysis, to explore the relationships between different variables and identify any significant predictors of menstrual disorders. By considering the limitations and potential solutions, future research can build upon this foundation and contribute to more comprehensive and effective strategies to improve menstrual health outcomes for women in the region.
Menstruation is considered an integral part of the life of women since it marks the beginning of their reproductive life. Lack of knowledge and awareness and proper hygiene practices during menstruation is associated with severe menstrual disorders. The findings of this study show that, among the PMS symptoms, change in mood, abdominal bloating, breast discomfort, etc., are the most common issues in the study population. The study also shows that dysmenorrhea is the most prevalent menstrual disorder, and menorrhagia is also quite common among women living in modern Dhaka. Though these women are educated enough, a large number of them still suffer from menstrual disorders because of a lack of cautiousness. According to this study, the reasons behind the prevalence of these disorders could be their food habits and their lifestyle. They like eating junk food while being somewhat aware of its detrimental effects on menstruation health. It highlights the necessity of targeted interventions and educational programs to promote healthier dietary choices and menstrual health awareness among young women. Moreover, there is a strong correlation between their food habit, lifestyle, and the prevalence of menstrual disorders. It is recommended that modern, young, and educated women should be made more aware of their menstrual health. From a policy perspective, the findings of this study can serve as a basis for developing targeted health interventions and awareness campaigns focused on menstrual health. Health policymakers should prioritize menstrual health education and hygiene promotion programs to empower women with knowledge about managing menstrual disorders effectively. These efforts can help improve the overall well-being and quality of life of women in Dhaka and beyond. As for researchers, this study sheds light on the existing gaps in knowledge about menstrual health in the context of modernized societies. Further research may delve deeper into the specific lifestyle and dietary factors that contribute to menstrual disorders. Longitudinal studies can help explore the long-term effects of menstrual disorders on women’s health and identify potential preventive strategies. This study can serve as a call to action for healthcare professionals to collaborate in raising awareness about menstrual health and supporting women in managing menstrual disorders.
