Multiple Drugs and Health Consequences in Diabetes Mellitus Type II
Bhattacharya AK, Rana K, Singh S, Bamaniya B and Sonkar CK*
Department of Medicine, Parul Institute of Medical Science & Research (PIMSR), Parul Sevashram Hospital, Parul University, Vadodara, Gujarat, India
*Correspondence: Chetan Kumar Sonkar, Department of Medicine, Parul Institute of Medical Science & Research (PIMSR), Parul Sevashram Hospital, Parul University, Vadodara, Gujarat, India
Received on 15 June 2021; Accepted on 30 July 2021; Published on 12 August 2021
Aim and Objective: To find the association between polypharmacy and health consequences in type 2 diabetes mellitus (T2DM). Materials and Methods: 50 patients with multiple drugs (two or more) and morbidity, glycemic control, macrovascular complications, hospitalization, gastrointestinal disorders, cost of medicine were studied. History, physical examination, relevant investigation, and consequences of drugs were also studied. Results: Male to female: 32:18; average age: 44 years. Findings were: hyperglycemia is seen in 34 patients, hypoglycemia in 2, retinopathy in 10, coronary artery disease (CAD) by electrocardiogram (ECG) and 2D echo in 12, old myocardial infarction in 3, renal function test abnormality in 6, stroke in 2, hypertension in 15, dyslipidemia in 13, hypothyroidism in 3, and hospitalization due to any of the above in 5. Conclusion: Diabetes, a metabolic disorder, due to chronicity leads to macrovascular and microvascular complications which in turn are compelled to increase the number of medications due to uncontrolled hyperglycemia. More than two-third of patients in our study showed uncontrolled hyperglycemia. Diabetes has multiple sites and mechanisms of altered physiological and pathological processes. It is practical to have the requirement of more than two drugs when blood sugar in diabetes is not controlled. Also, it is obvious that the simultaneous use of more than one drug-having different mechanism of action appears to have an impact on treatments to control hyperglycemia. Sometimes, multiple drugs/therapy may give rise to undesirable side effects and it may be due to drug-drug or disease drug interaction. Furthermore, the activity of multiple targets by multiple drugs requires additional study. Multiple drugs in diabetes were seen more in males with geriatric age groups. Main reasons being comorbidities, which may be the main cause of morbidity and mortality, especially CAD, heart failure and diabetic cardiomyopathy. There is an indirect relationship between the glycemic control and the development and progression of clinical manifestations of comorbidities. Various comorbid diseases in diabetes require concomitant medications, that increases pill burden. Tailoring medical therapies to the patient’s biological characteristics may help to optimize disease treatment, thereby improving overall prognosis and decreasing comorbidities’ risk. Appropriate exercise and diet may reduce hyperglycemia with reduction in pill burden.
Keywords
diabetes mellitus, glycemic control, health consequences, multiple drugs, polypharmacy
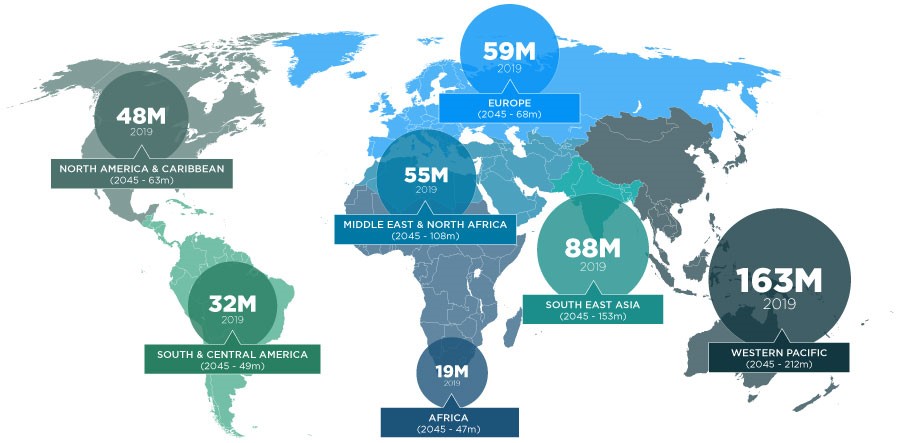
Diabetes Mellitus (DM) is a metabolic syndrome having multiple etiological factors characterized by chronic hyperglycemia with disturbances in carbohydrate, protein and fat metabolism resulting from defects in insulin secretion, action or both [1]. Diabetes prevalence around the globe is estimated to be 9.3% (463 million people) in 2019 and is expected to reach 10.2% (578 million) by 2030 and 10.9% (700 million) by 2045 (Figure 1). Prevalence of impaired glucose tolerance globally is estimated to be 7.5% (374 million) in 2019 and forecasted to reach 8.0% (454 million) by 2030 and 8.6% (548 million) by 2045 [2]. There has been a claim of about ~4 million adult deaths due to diabetes in 2017 of which more than 75% people live in lower and middle-income countries. In the world, India is considered as the “diabetes capital”; a home to 74 million diabetics with a prevalence of ~8.7% among the adult population [3]. It is one of the leading causes for premature deaths when improperly managed and can lead to various health issues including heart disease, stroke, kidney disease, blindness, nerve damage, leg and foot amputation and death [4].
Figure 1: Prevalence of diabetes.
The complications are classified as macrovascular and microvascular, which are increasing worldwide aggregating to major health problems in developing and developed countries. Alteration in microvascular function may arise even before overt hyperglycemia and vascular pathologic changes manifest [5]. Several landmark studies such as United Kingdom Prospective Diabetes Study (UKPDS) have demonstrated that strict glycemic control does limit microvascular diseases while attempts to improve macrovascular outcomes through glucose lowering interventions [6].
Polypharmacy means the usage of multiple medicines [7]. In the United States, among people suffering from type 2 diabetes mellitus (T2DM), 54% of the cases were found to have an association with polypharmacy [8]. Adverse drug reaction, drug-drug and drug-food interactions can be characterized by an increased daily intake of drugs [9]. For the management of DM and its complications, avoiding polypharmacy not only may improve target outcome for the patients but also contributes in the addition of unessential medication to the drug regimen [10]. It may not have a positive effect on the patient, their family, health system and economy and also adversely effects their adherence to medicines, quality of life and life expectancy and can lead to minimal blood glucose control and hospital admission [8, 11, 12]. Many factors leading to the risk of polypharmacy in the patients include multiple care providers, ageing population, complex drug therapies, multiple chronic condition in a single patient and adverse drug reactions. Elderly adults are having a high risk of receiving polypharmacy [13].
Materials and Methods
In Parul Sevashram Hospital attached to Parul Institute of Medical Science & Research (PIMSR), an observational study was carried out in the duration of 14 months from January 2018 to February 2020 for 50 patients after getting approval from Institutional Ethics Committee.
The data was collected with all the information about the patient’s complaints, consequences of drugs and the laboratory results in the Case Record Form which was predesigned and the analysis is made from the data provided.
Observation was carried out to find out the scope of the study in the Parul Sevashram Hospital.
Relevant literatures were reviewed.
Data of the patients was collected and recorded in the Case Record Form and analysed the consequences of polypharmacy in diabetic patients.
Study criteria
Inclusion criteria
Patients of either gender between the age group of 20–70 years of age (both years inclusive)
Patients with known case of T2DM for the minimum of 2 years
Patients on more than or equal to 2 medications
Exclusion criteria
Lactating and pregnant woman or planning to become pregnant
Patients with diabetes mellitus type 1
Unwilling patients/psychiatric patients
Other disease conditions or laboratory parameters as per investigators discretion
Biophysical estimations
Medical/medication history, physical examination, vital signs, laboratory investigation- RBS, HbA1C, ECG, 2D echocardiography (if required), renal function test, relevant investigations and consequences of drugs were studied and recorded.
Statistical analysis
The data was represented graphically in MS-Excel with median values.
Results
During the study period, 50 patients were examined, interviewed and their prescriptions were studied. The patients were analyzed and the main characteristic of this study was the relation between polypharmacy and the health consequences with the help of history, physical examination and laboratory investigation.
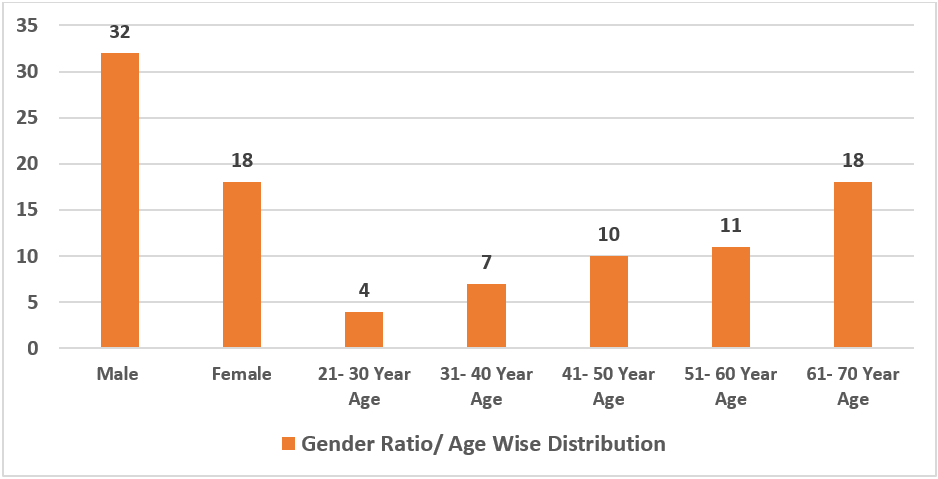
Out of the 50, there were 32 males (64%) and 18 females (36%). Median age of the patients in the study population ranged from 20–70 years. The average age of the study population was 58 years. About 21–30 years were 4 (8%), 31– 40 years were 7 (14%), 41–50 years were 10 (20%), 51–60 years were 11 (22%), 61–70 years were 18 (36%) (Figure 2). So, it can be concluded that as the age increased, the level of comorbidity in relation to patient’s age increased. The present study revealed elderly patients suffering from T2DM had a greater risk of suffering from macrovascular and microvascular complications which leads to polypharmacy.
Figure 2: Gender ratio/age wise distribution of patients.
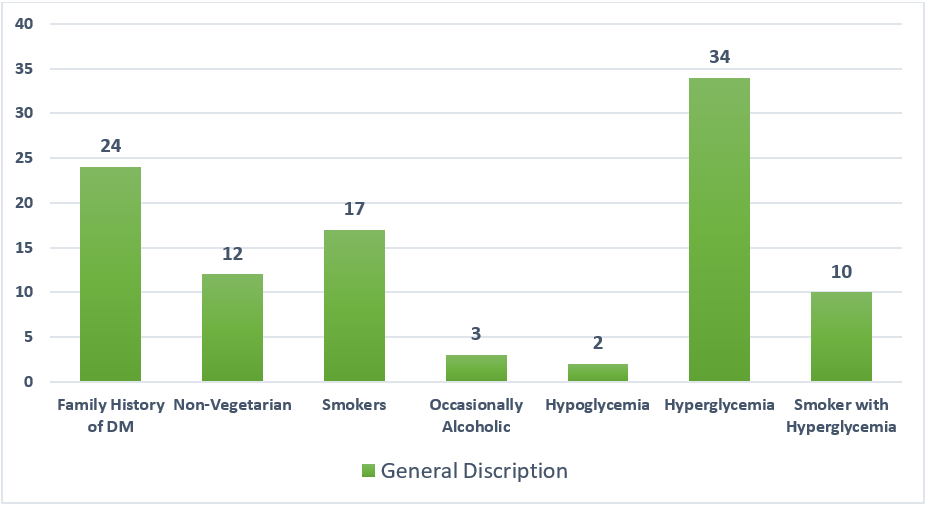
With a study population of 50 patients, 24 (48%) patients were having family history of diabetes, 12 (24%) patients claimed that they were non-vegetarian, 17 (34%) of them were smokers, and 3 (6%) of them consumed alcohol occasionally. Hypoglycemia in 2 and hyperglycemia was seen in 34 (68%) patients. In this study, out of 34 patients having hyperglycemia, 10 were smokers. Smoking causes inflammation and increases oxidative stress leading to insulin resistance which can further lead to macro and microvascular complications.
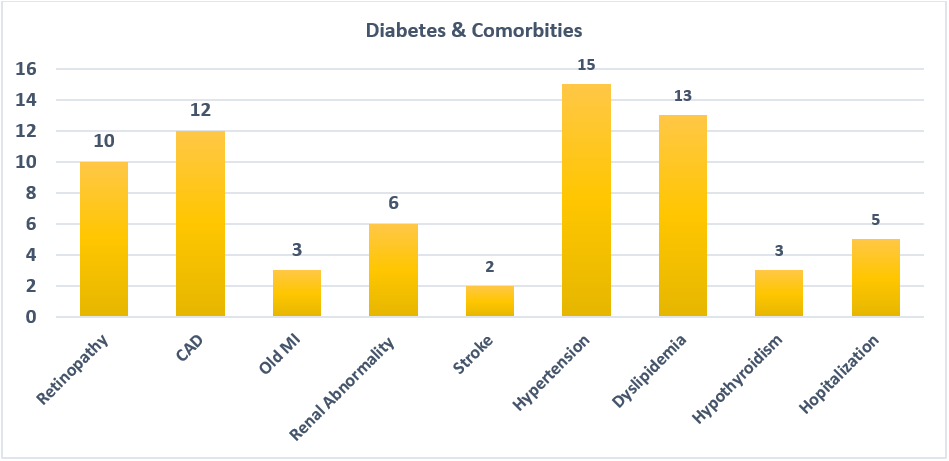
Diabetic patients suffered from various comorbidities: retinopathy in 10 (20%), coronary artery disease (CAD) by ECG and 2D Echo in 12 (24%), old myocardial infarction (MI) in 3 (6%), and renal function test abnormality in 6 (12%).
Stroke in 2 (4%), hypertension in 15 (30%), dyslipidemia in 13 (26%), hypothyroidism in 3 (6%), and hospitalization due to any of the above in 5 (10%). Dyslipidemic patients had high plasma triglyceride concentration and LDL cholesterol. 8 patients with hyperglycemia had high triglycerides. Therefore, these patients were at a higher risk of having cardiovascular complications, stroke in the future (Table 1) (Figure 3 and 4).
S. No
Complications
No. of Patients (N = 50)
1.
Hyperglycemia
34
2.
Hypoglycemia
2
3.
Hyperglycemia with smoking
10
4.
Retinopathy
10
5.
Coronary artery disease
12
6.
Old myocardial infraction
3
7.
Renal abnormality
6
8.
Stroke
2
9.
Hypertension
15
10.
Dyslipidemia
13
11.
Hypothyroidism
3
12.
Hospitalization (any reason)
5
Table 1: List of complications.
Figure 3: General description of the study population.Figure 4: Diabetes and comorbidities.
This study suggested that the level of polypharmacy increased with the age of patients and the maximum was in the age group of 61–70 years.
Along with the modern medicines, use of alternative medications was also seen. This study estimated that 5 (10%) patients consumed homeopathic medicines and 6 (12%) patients consumed Ayurveda drugs parallel to the allopathic medicines.
Discussion
Diabetes, a metabolic disorder often leads to various disease-related complications i.e., macrovascular and microvascular complications which in turn are compelled to increase the number of medications. Polypharmacy leads to an increase in the pill burden and can further lead to various other complications. The objective of our study was to evaluate the impact of polypharmacy in diabetic patients aged 20–70 years in the Vadodara district. This study revealed that the number of drugs were between 3–10 in each patient.
From this study, it is evident that the polypharmacy increased with an increase in the age and was seen majorly in the elderly patients i.e., the geriatric age group of 61–70 years. There were 64% males, 36% females and the average age was 58 years. A similar study by Upadhyay DK et al estimated that 59.59% of the study population were males and 43.41% were females [14]. The present study reveals that the prevalence of diabetes was more in males. This study evaluated that the study population suffered from at least one common condition, i.e., hypertension (30%) or dyslipidemia (26%). DM is associated with a considerably high risk of premature atherosclerosis, particularly coronary heart disease (CHD) and peripheral arterial disease [15, 16]. Also, there is an association between atherosclerotic cardiovascular disease and high serum cholesterol and triglyceride levels in both type 1 and type 2 diabetes [17, 18]. In diabetics, both hypertension and dyslipidemia increase the chances of cardiovascular diseases. Researches show that around 80% of diabetic patients die because of cardiovascular disorders [19].
According to the American Diabetes Association, the target fasting glucose values range from 80–130 mg/dl and postprandial blood sugar levels are targeted at < 180 mg/dl. Therefore, levels of fasting blood glucose > 130 mg/dl and postprandial level > 180 mg/dl are considered as having poor control [20]. Based on this definition, the present study revealed that 68% of the patients had uncontrolled diabetes (hyperglycemia). Of the hyperglycemic patients, 10 were smokers. However, both the American Diabetes Association and the International Diabetes Foundation do not currently include smoking as a modifiable risk factor for diabetes development or consider smoking status as a factor that should be prompted in the diabetes screening [21, 22]. 20% of the patients having retinopathy suffer from DM which is the most common complication. There is an indirect relationship between glycemic control and the development and progression of diabetic retinopathy (DR). A decrease in glycosylated hemoglobin levels was associated with a significant decrease in the progression of DR [23]. 4% of the patients involved in the study had a stroke. T2DM is a lifestyle disorder, it has additional risk factors in future like stroke, obesity, hypertension and dyslipidemia [24]. 6% of the patients suffered from hypothyroidism and there are studies that suggest that thyroid hormone therapy can be looked at as a therapeutic strategy to alleviate diabetes and atherosclerosis. 24% of patients had CAD and 6% had old MI. DM is independently associated with the development of heart failure. The increase in the myocardial vulnerability in diabetes along with other risk factors may be responsible for distinct cardiomyopathy specific to diabetes, termed diabetic cardiomyopathy [25].
It is true that literature studies in various parts of the world suggests that diabetes is associated with various comorbid diseases and requires concomitant medications. However, among 91 million people residing in West Bengal, the prevalence of diabetes is quite high, about 12% in Kolkata and 13% in Howrah [26]. This study tried to evaluate the co-morbidity which leads to polypharmacy in diabetes patients. So, by reducing the pill burden and providing maximum benefit to the patients is most important. Also, more research is required on the pharmacokinetics and pharmacodynamics of appropriate and scientific fixed drug combinations. Therefore, delicate balance is required to add drugs, control the disease and avoid adverse drug effects. There is a need for critical decision to tilt the balance of benefits in favor of the patients when adjuvant therapy is required and to avoid side effects of multiple medicines being prescribed.
Conclusion
Diabetes, a metabolic disorder, due to chronicity leads to macrovascular and microvascular complications which in turn are compelled to increase the number of medications due to uncontrolled hyperglycemia. More than two-third of the patients in our study showed uncontrolled hyperglycemia.
Diabetes has multiple sites and mechanisms of altered physiological and pathological processes. It is practical to have the requirement of more than two drugs when blood sugar in diabetes is not controlled. Also, it is obvious that the simultaneous use of more than one drug-having different mechanism of action appears to have an impact on treatments to control hyperglycemia. Sometimes, multiple drugs/therapy may give rise to undesirable side effects and it may be due to drug-drug interaction or disease drug interaction. Furthermore, the activity of multiple targets by multiple drugs requires additional study.
Multiple drugs in diabetes were seen more in males with geriatric age groups. Main reasons being comorbidities, which may be the main cause of morbidity and mortality, especially CAD, heart failure, and diabetic cardiomyopathy. There is an indirect relationship between the glycemic control and the development and progression of clinical manifestations of comorbidities. Various comorbid diseases in diabetes require concomitant medications, that increases pill burden.
Tailoring medical therapies to the patient’s biological characteristics may help to optimize disease treatment, thereby improving overall prognosis and decreasing comorbidities’ risk. Appropriate exercise and diet may reduce hyperglycemia with reduction in pill burden.
Limitations
Small sample size
Unavailability of funds
Study includes one geographical location only
Single-arm study that needs a control group
Recommendation
Need to follow up the same patient group for a long time (cohort study). A large sample size (robust) is needed to substantiate the objective of the study.