diffusion-weighted imaging, MRI, infarction, imaging
DWI: diffusion-weighted imaging; MRI: magnetic resonance imaging; ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery; TIA: transient ischemic attack
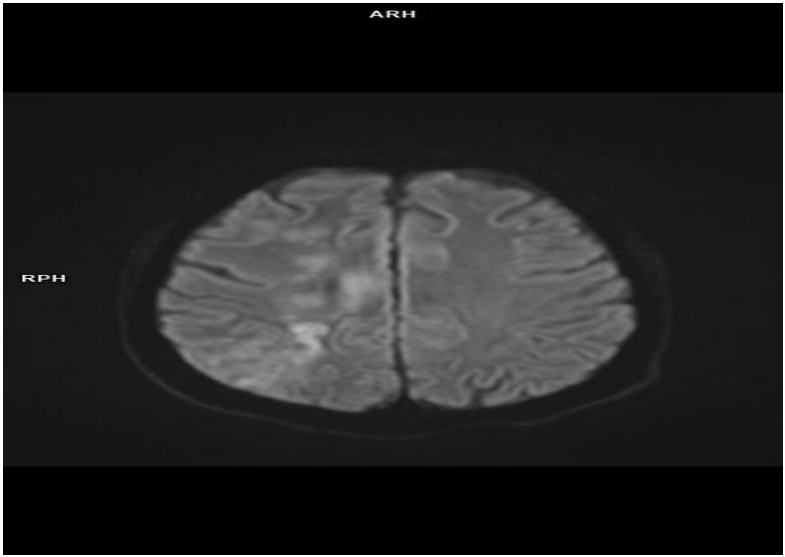
Diffusion-weighted imaging (DWI) sequence MRI endocranial image showing both cortical external and subcortical internal non-homogenous hyperintensity confluent focal diffusion restriction fields corresponding to components of complex unilateral right watershed infarctions (axial section) – multi-infarct changes located in the right parieto-occipital, right frontal, and parietal lobe as part of the so-called complex watershed cerebral infarcts (both right ACA and MCA and right MCA and PCA irrigation supply territories – the latter is predominant). Diffusion and perfusion imaging is considered the best and most sensitive imaging tools for these lesions’ early detection and characterization mainly because the DWI sequence better depicts not only the location of the border zone infarcts in relation to the vessels but also enables quite successful differentiation between acute, subacute, and chronic strokes and very often before such changes are apparent on conventional MRI sequences (T1w, T2w, FLAIR, etc.) and/or become clinically apparent and visible. Generally, one of the most valuable DWI clinical applications is the early detection of brain infarction (ischemic and hemorrhagic). DWI can be positive for hyperacute cerebral infarctions even less than 30 min from the onset of earliest clinical symptoms. Also, in the first 6–7 h from the onset of earliest clinical symptoms, DWI is still undeniably considered a fast superior, and far more sensitive imaging technique compared to T2w and FLAIR sequences and is considered the main imaging technique and sequence for this pathology detection (93–98% sensitivity compared to 55–58% of conventional MRI sequences). Even 17 days after the stroke, ischemic lesions could have high signal intensity on the DWI sequence. Still, radiologists should also remember that false positive results were reported (TIA, epileptic seizures and fit, multiple sclerosis demyelinating lesions and plaques, encephalitis, hypoglycemia, mitochondrial encephalopathy, lactic acidosis, stroke-like episodes, transient global amnesia and the number of other conditions). The imaging, therefore, needs to be interpreted in the light of the clinical picture and manifestations and DWI should not be regarded as a completely specific technique for ischemia.
The main DWI physical principle is to focus on movements and particularly and more precisely said micromovements (random, Brownian micromovements) of the water molecules inside voxels. In contrast, extracellular water is the main object of evaluation and exploration in diffusion imaging. Data provided by DWI are indirect pieces of information regarding the structure surrounding these water molecules. DWI offers unique functional information on water molecular diffusion physical properties; these pieces of information could be further used for collecting important information and studying lesion cellularity and cell membrane integrity. DWI MRI images can be evaluated by observing signal intensity changes on b-value images usually concomitantly reviewing ADC maps and getting conclusions after careful evaluation of both sequences. Fusion of high b-values with anatomical images has been found to aid in lesion detection and appears to be very helpful in lesion localization and at least to some degree in lesion characterization. DWI MRI images can presumably be very helpful for both lesion detection and localization because they incorporate two very important differences and contrast mechanisms: increased water content and impaired water diffusivity, both of which increased signal intensity and conspicuity of hypercellular changes (ischemic lesions, tumors, etc.) on high b-values images. An inverse correlation between minimal ADC values and lesion cellularity has been verified by pathohistology in a wide variety of both ischemic and neoplastic changes. The greater the density of structures that hinder and impede water mobility, the lower the ADC values are, and vice versa. Following that, ADC values are considered a very important quantitative noninvasive indicator and imaging biomarker of cellularity and/or cell density. Diffusion-weighted MR imaging was performed in this case using high-speed, single-shot EP techniques with TR 6000, TE 144, matrix 96 × 128, FOV 23.3 × 31, and five b values of 0, 160, 360, 640, and 1,000 s/mm2.
A 57-year-old male respondent, after an initial physical examination, was sent in an urgent ambulance to Urgent Medicine, Neuroradiology Department suspected of clinical neurological signs of left-sided weakness and dysfunction in the form of paralysis (both left-sided hand and accompanying leg weakness), with hard walking and quite difficult interpersonal communication, that occurred approximately a few days (5–6 days) before initial hospital administration.
As watershed or border zone infarctions quite often are burdensome neuroradiological both diagnostical and therapeutic conundrum and considering that particularly internal border zone infarcts which (located between the anterior and middle cerebral, ACA and MCA perforating arteries – their deep and superficial branches more precisely) have a high predilection for future cerebrovascular major events (initial and recurrent strokes, TIA, hemorrhagic transformations, etc.) and different morbidity and invalidity due to minor chance of developing quick adequate collateral supply (mainly because perforating arteries are terminal branches and in watershed infarctions multiple concomitant microembolus are present at the same time), prompt recognition and complex multidisciplinary therapy (pharmacology, interventional radiology, and/or vascular surgery, etc.) in order to decrease irrevocable ischemic changes (core ischemic infarcts) is crucial and neuroradiologists should keep in mind and recognize these types of ischemic lesions because they can be present in up to 12% of all documented central nervous system infarcts. Thus, DWI is a useful method that can detect neurologically silent, subtle, and/or asymptomatic ischemic lesions.
