Abstract
Over the past ten years there have been guidelines that have been produced regarding the management of individuals with diabetes undergoing a surgical procedure. This clinical audit will be focusing on the area of orthopaedics and the standards of care received by individuals with diabetes. The audit examined retrospectively; the care received in a large acute NHS trust with a sample of 78 adult individuals with diabetes. Ten audit criteria were reviewed and evaluated and compared to the guidance that is currently available nationally. Both emergency and elective procedures were assessed to see if there were any variances in the management of individuals with diabetes. On review of the results, a number of recommendations will be put forward to the trust with regards to changes that should be implemented to enhance patient care.
Keywords
diabetes, orthopaedics, standards
Abbreviations
DISN: a diabetes specialist nurse that works within the hospital setting, caring for inpatients; DKA: diabetic ketoacidosis – occurs when there is a severe lack of insulin in the body; HbA1c: glycated haemoglobin – used for diagnosing diabetes. An HbA1c 42–47 mmol/mol diagnoses pre-diabetes and anything over 48 mmol/mol is diagnostic of diabetes (which could be either type 1 or 2); Pre-operative: occurring in the period before a surgical operation; Peri-operative: occurring at or around the time of a surgical operation; Post-operative: occurring in the period after a surgical operation; VRIII: variable rate intravenous insulin infusion – intravenous insulin alongside intravenous glucose-based fluids to manage hyperglycaemia. Usually used when an individual will be missing more than one meal; LOS: length of stay
Introduction
There are currently 4.7 million people who have diabetes living in the UK. This figure is predicted to rise to 5.5 million by 2030 [1].
Recent data from the National Diabetes Inpatient Audit (NADIA), showed that 18% of inpatients have diabetes [2]. More than 15% of patients undergoing surgical procedures under the NHS are known to have diabetes [3]. This equates to approximately 323,000 operations within the UK each year [4].
With the number of cases of diabetes set to increase, the number of individuals with diabetes undergoing surgery will therefore also increase.
Surgery can lead to metabolic stress which can cause an increase in catabolic hormone secretion and an inhibition of anabolic hormones such as insulin. Often, postoperatively, this is followed by a period of insulin resistance which can lead to hyperglycaemia [5].
Individuals with diabetes who undergo surgery are known to have greater complication rates, mortality rates and length of hospital stay [6]. This may, in part, be due to the fact that around 15% of individuals with diabetes, have an HbA1c of greater than 69 mmol/mol pre surgery [7].
It is recommended that an individual’s preoperative HbA1c level is optimised, at least three months prior to any elective surgery. This, however, has been found to only be achieved in around 35% of patients [8]. Individuals with poor glycaemic control prior to surgery are more likely to remain hyperglycaemic for the perioperative period, therefore increasing their risk of post-operative infections and poor wound healing [9]. There is widely published data showing link between hyperglycaemia in hospitalised patients and poor outcomes [10].
The landmark UKPDS study [11] demonstrated that intensive blood-glucose levels achieved with either sulphonylureas or insulin decreased the risk of microvascular complications, in individuals with type 2 diabetes. It did also show however that intensive treatment increased the risk of hypoglycaemia. This increased risk of hypoglycaemia has been shown in several random control trials (RCTs) including NICE-SUGAR, have shown that intensive glycaemic management for these patients has resulted in severe hypoglycaemia [12]. Within this trial, the 90-day mortality rate was found to be significantly higher within the individuals who were intensively treated compared to those individuals undergoing conventional therapy. For this reason, research has been ongoing within the area of perioperative care for a number of years.
Due to the increase in complication rates, individuals with diabetes are often classified as being at high risk, meaning many are prevented from undergoing day surgery and are admitted the day prior to surgery [13].
According to Moghissi et al. [10], excess bed days for individuals with diabetes within surgical wards were estimated to be 45% greater than for individuals with diabetes admitted to medical wards. Re-admission rates post operatively are also found to be more frequent with individuals with diabetes [14].
Frisch et al. [15] report that the perioperative mortality rate in individuals with diabetes is up to 50% higher than those who do not have diabetes. Wallace et al. [16] go as far as to say that the perioperative environment is a hazardous setting for individuals with diabetes. This has led to a number of publications being produced with regards to the management of individuals with diabetes who are undergoing surgery. These include the Association of Surgeons of Great Britain and Ireland [17], Association of Anaesthetists of Great Britain and Ireland [18], Joint British Diabetes Society (JBDS) [19] and British Association of Day Surgery (BADS) [20]. Due to the issues highlighted above, a report was carried out looking at where care could be improved for individuals with diabetes who were undergoing surgery. The report, by the National Confidential Enquiry into Patient Outcome and Death (NCPOD) [21], showed a lack of clinical continuity of diabetes management across the different specialties in the perioperative pathway. This report drew attention to the fact that 14% of patients did not have adequate blood glucose monitoring during theatre which led to hypoglycaemia occurring in 4.7% of these patients. McCavert et al. [22] showed that following hospital protocols in relation to glycaemic control led to a 25% reduction of perioperative complications.
The most recent guidance is from the Centre for Perioperative Care (CPOC) [23], and this draws from findings from the previous guidance listed above but from a more practical ‘hands on approach’ for patient care. It also considers the findings from the Getting It Right First Time (GIRFT) programme and emphasised the need to promote self-management for individuals with diabetes. This is due to individuals often feeling disempowered with regards to the management of their diabetes in hospital [24]. The self-management of insulin within hospitals is an area of work that has been highlighted as a way of empowering individuals with diabetes to have more control over their diabetes management in hospital. This is an area that the author has implemented within their own NHS trust [25].
Medication errors were shown to have occurred in around 1/3 of inpatients with diabetes in the last NADIA report [2], with these errors occurring more commonly in surgical wards compared to those in medical wards.
Insulin is the medication most frequently involved in medication errors. Due to this, insulin has been categorised as one of the top five high risk medications within the inpatient setting, which is why it remains as one of the medications included in NHS England’s ‘Never events’ [26] (Appendix 1).
Insulin omission in individuals with type 1 diabetes in hospital is unfortunately all too common. This has led to one in every 25 inpatients with type 1 diabetes developing diabetic ketoacidosis (DKA) within the hospital setting [2].
The National Service Framework (NSF) for diabetes [27] concluded that inpatient services could be improved if an inpatient diabetes team were in place. Inpatient length of stay (LOS) for individuals with diabetes was shown to be reduced, whatever the reason for admission, if the patient was reviewed by a diabetes inpatient specialist nurse (DISN) [28].
For individuals who undergo an elective procedure, a pre-operative assessment should be arranged. Within this assessment, Barker et al. [6] suggests that a plan should be made which minimises the time that the individual needs to be fasted, such as being booked into the first operating slot of the morning list. Barker et al. [6] go on to recommend that written instructions with regards to the medications patients need to take or omit on the day of surgery should be provided to each patient. Wallace et al. [16] have concluded that there are three main themes with regards to the management of individuals with diabetes who are undergoing a surgical procedure that have become apparent within their systematic review. They examined the management of patients with diabetes with regards to perioperative pathways. These themes were;
- poor patient outcomes,
- increased length of stay
- lack of adherence to guidance or protocols and glycaemic control.
There have been national and local guidelines that have been developed to address this area of care, that have been borne out of research that has shown poor outcomes for patients. There is, however, great variability in practice [29] and globally, diabetes management during the perioperative period is widely debated [16].
Franco et al. [29] highlight the importance of formal guidelines and state that without standards, there can be no improvement. Hommel et al. [30] conversely suggest that it is unknown whether these guidelines lead to optimal or ‘good’ quality care delivery.
The area of perioperative care is a complex and multidisciplinary process [30]. For optimal diabetes care, the specific needs of the individual with diabetes should be taken in account, prior to admission, during the admission and through to discharge. There is limited research concentrating on specific areas such as orthopaedic surgery, even though individuals with diabetes are more likely to require orthopaedic surgery than individuals without diabetes [31], in particular foot and ankle surgery [32].
Negus et al. [33] published a recent review highlighting the need for trauma and orthopaedic surgeons to be aware of the increased risks of complications when operating on individuals with diabetes. Diabetes in itself is a risk factor for suboptimal outcomes in the perioperative period in individuals undergoing orthopaedic surgery [34].
Infection rates were shown to occur in 71% of individuals with diabetes compared to 19% in individuals without diabetes [33]. Increased LOS and a higher perioperative mortality rate have also been recognised in a number of studies [29, 30, 34]. Levy et al. [4] suggest the perioperative mortality rate for individuals with diabetes is up to 50% higher than in individuals without diabetes.
A study quoted by Wukich [32] reviewed 1166 individuals who were admitted due to an orthopaedic cause. Three hundred and eighty-five patients had an admission blood glucose of >120 mg/dL (6.7 mmol/l) and only 45% of these were known to have diabetes prior to admission. This highlights the need for all patients to have their blood glucose levels checked within the secondary care setting.
There is much debate regarding the optimal HbA1c level when undertaking a surgical procedure. Underwood et al. [35] assert that due to lack of data, arbitrary HbA1c cut-offs are used by health care professionals within perioperative care. Negus et al. [33] however, found that individuals with a HbA1c > 53 mmol/mol were five times more likely to develop post-operative infections than individuals with a HbA1c < 53 mmol/mol. Akiboye and Rayman [31] agree and state that higher rates of surgical site infections are found in individuals with a HbA1c > 53 mmol/l.
Several pieces of literature regarding orthopaedic surgery suggest an optimal HbA1c of below 68–75 mmol/mol [36]. It is recommended that surgery should be delayed allowing optimisation of glycaemic control if an individual’s HbA1c is above this [30]. Rizvi et al. [34] agree stating that elective surgery should be delayed in order to obtain satisfactory glucose control – suggesting a HbA1c < 53 mmol/mol. Dhatariya et al. [3] have a slightly higher threshold and state that if the individuals HbA1c is > 69 mmol/mol then they should be referred to the diabetes specialist team for advice. This is supported by Barker et al. [6].
The risk of hyperglycaemia is well documented as a cause for increased complications in the perioperative period. Within the field of orthopaedics, preoperative hyperglycaemia has been associated with an increased incidence of prosthetic joint infections [33]. This is also true for total knee arthroplasty and total hip arthroplasty [34]. It is estimated that between 5–30% of inpatients have diabetes and hyperglycaemia.
Reich et al. [36] demonstrated how the admission blood glucose was a good predictor for the risk of a surgical site infection, with elevated levels putting the individual at a higher risk.
A blood glucose of 6–12 mmol/l is generally the standard target used in the inpatient setting and this is what is recommended by the JBDS [19]. Acceptable levels from 4–12 mmol however are advocated in other guidance such as the association of anaesthetists of Great Britain and Ireland [18].
It is clear from the literature that it is difficult to simply reduce glycaemic levels without causing an increased risk of hypoglycaemia. It is generally agreed that hypoglycaemia should also be avoided due to the potential complications that could arise [32].
Page et al. [37] found that due to inadequate blood glucose monitoring, intra operative hypoglycaemia occurs in 4.7% of individuals with diabetes whilst Levy et al. [4] claim that 22% of inpatients with diabetes will have at least one episode of hypoglycaemia during their admission.
The majority of the guidance that has been published nationally focus on the area of elective surgery. This enables health care professionals to have a number of weeks where they are able to optimise an individual’s HbA1c and diabetes management prior to the surgery. This is in comparison with emergency surgery where there may be a few hours to make plans at best. This being said, Page et al. [37] claim that although it is recommended that an HbA1c level is checked three months prior to surgery, this only occurs in 35% of individuals. Dhatariya et al. [3] suggests that for emergency surgery, if the individuals blood glucose rises above 10 mmol/l, that a variable rate IV insulin infusion (VRIII) is commenced. A HbA1c on admission is also beneficial as this can influence subsequent diabetes management following the surgery, however according to Wallace et al. [16], this only occurs in 52% of individuals. Wallace et al. [16] found that emergency patients had a significantly longer LOS than elective patients. Early involvement of the diabetes specialist team is also appropriate for individuals who are classed as high risk. Where possible, pre assessment should be carried out for all individuals undergoing a surgical procedure, whether or not they have diabetes. Dhatariya et al. [3] suggest that sub-optimal glycaemic control needs to be addressed prior to the referral for surgery and that this requires careful planning, involving the patient at all stages. Hommel et al. [30] however, demonstrated within their research that only 33% of individuals with diabetes were involved in the decision making regarding their diabetes management.
It is well documented that individuals with diabetes who are undergoing surgery should be placed at the top of surgical theatre lists. This minimises the period of starvation needed [33]. JBDS guidance [19] suggests that 95% of individuals with diabetes should be allocated a place in the top third of theatre lists. Individuals who miss more than one meal should be managed using a variable rate intravenous insulin infusion (VRIII). Rizvi et al. [34] suggest that this should be the case for all major orthopaedic surgery, and that it should be commenced 2–3 h prior to allow titration to the desired glucose range.
Insulin errors are unfortunately all too common within the inpatient setting. They are usually caused by inadequate knowledge, timing of administration and lack of dose verification requirements [34]. For this reason, insulin continues to be part of the Department of Health’s list of ‘never events’ [38]. In the recent NADIA audit, medication errors were found to have occurred in around 33% of individuals with diabetes, with these being more common in surgical ward areas [2].
A staggering 1 in 25 inpatients with type 1 diabetes develop DKA during their admission, often due to insulin omission [39]. Franco et al. [29] suggest that an algorithm can be used to assist health care professionals on how to adjust medications in the days prior to surgery. Within their guidelines, Barker et al. [6] provide useful guidance for the perioperative adjustment of insulin and oral hypoglycaemic agents.
Diabetes UK [39] stipulate that all hospitals should have multidisciplinary inpatient diabetes team. They go on to state how 28% of individuals with diabetes who needed to see a specialist diabetes team were unable to. Negus et al. [33] champion the involvement of diabetes specialist teams early. Akiboye and Rayman [31] agree and acknowledge the fact that diabetes specialist nurses can considerably reduce LOS, thereby demonstrating significant cost saving implications. Dhatariya et al. [3] concur and suggest that clear guidelines need to be in place to identify when a patient should be referred to the diabetes specialist team. Moghissi et al. [10] showed that the input of diabetes specialist teams resulted in a 56% reduction of LOS. The perioperative environment is a hazardous setting for individuals with diabetes [16]. Page et al. [37] agree stating that diabetes is frequently ignored prior to surgery and that glycaemia is often mismanaged during the admission which can lead to frequent post-operative complications. Even with protocols in place, Wallace et al. [16] found that 60% of elective patients with type 1 diabetes were not treated according to the hospital protocol.
As well as the importance of following guidelines, education for all levels of surgical care professionals is essential and advocated by Rizvi et al. [34].
It is clear from the review of current literature that the standards of care received by individuals with diabetes varies due to differing opinions of the optimal management within the inpatient setting. Further research is required within the field of orthopaedic surgery to review whether the current available guidelines are being adhered to and to assess the barriers that may be in place.
Methodological Approach
An audit was the approach the author chose to use to review the standards of care received by people with diabetes who undergo orthopaedic surgical procedures within a secondary care setting. Clinical audit is carried out to find out if healthcare is being provided in line with standards and informs care providers and patients where their service is doing well, and where there could be improvements [NHS England, 26]. Shankar et al. [40] state that the purpose of clinical audits is to generate findings that will benefit patients and their care delivery. The Healthcare Quality Improvement Partnership (HQIP) promote quality in healthcare, particularly trying to increase the impact of clinical audit on healthcare quality improvement [41]. They support healthcare professionals to review and improve clinical practice, such as the author is undertaking. This approach was chosen as clinical audits are a valuable tool in order to improve quality of care for individuals with diabetes. The aim of this audit was to improve inpatient care and suggest changes that could be made to further enhance the patient experience. There were three key guidelines available to compare standards, so the author used these to compare how their trust compared to these.
Audit setting
The setting used for the audit was a large acute NHS teaching hospital which is also a major trauma centre. The bed capacity is approximately 1300 and there is a 16.8% prevalence of diabetes in the inpatient population [42]. 166 individuals with diabetes underwent an orthopaedic procedure during the audit period.
Ethical and governance issues
The Caldicott Committee [43] was established for the protection and the use of patient information. They created a number of recommendations which included ensuring that the minimum necessary patient identifiable information is used. Within the audit, only data relevant to the audit criteria was collected and this was anonymised on an excel spreadsheet. This data was stored on a password protected USB that only the author had access to. The audit was registered within the authors trusts audit data base and was discussed with stakeholders which included the orthopaedic governance department, lead clinicians and the inpatient diabetes team. This ensured that the appropriate approvals were in place prior to the audit being undertaken.
From the audit outcomes, ten audit criteria were developed (Table 1).
| Audit criteria | Target | Exceptions | Source of evidence |
| 1 | Individual was referred for diabetes specialist team review if HbA1c > 69 mmol/mol | 100% | If the individual has frail/elderly and had a higher individualised HbA1c target | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 2 | Diabetes type was documented on admission | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 3 | A medicines reconciliation was documented on admission | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 4 | A medication plan was made for pre, during and post procedure | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 5 | The timing of surgery was considered (e.g., prioritised to minimise fasting) | 100% | The surgery was an emergency | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 6 | A VRIII was used if the patient was missing more than one meal | 100% | Evidence of significant hypoglycaemia | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 7 | Individuals with type 1 diabetes received insulin at all times | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 8 | Blood glucose levels were maintained between 6–12 mmol/l during the admission | 100% | If the individual was frail/elderly and had a higher individualised blood glucose target | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 9 | Ketone levels were monitored if indication (e.g., type 1 diabetes or significant hyperglycaemia) | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
| 10 | Individuals were referred to the inpatient diabetes specialist team according to their criteria | 100% | – | JBDS (2011) NCPOD (2018) and CPOC (2021) |
Table 1: Audit criteria developed from the audit outcomes.
There are three main guidelines that have been developed within the United Kingdom with regards to care of individuals with diabetes undergoing a surgical procedure that were used to compare against the care received by the patients within the audit. These are by JBDS [19], NCPOD [21] and CPOC [23].
An audit protocol was developed by the author to highlight the aims and objectives for the audit and to outline the methodology and data collection methods. A strict audit inclusion/exclusion criteria was documented to ensure the relevant data was captured.
Retrospective data was used due to the Covid-19 pandemic as the author wanted to review the usual standards of care within their trust for individuals undergoing both emergency and elective procedures. A large percentage of elective surgery was cancelled during the pandemic so this would have affected the individuals that the author would have been able to include within the audit.
The audit population includes adults with either type 1 or 2 diabetes taking oral or injectable therapy. Both males and females were included within the audit and adults of all ages were included. All orthopaedic procedures were included as long as they required the individual to be fasted and an overnight stay in hospital. This ensured that medication and monitoring post procedure could be included within the audit (Table 2 and 3).
| Title | Standards of care received by people with diabetes who undergo orthopaedic surgical procedures within a secondary care setting: a clinical audit. |
| Methodology | Retrospective audit Information from patient records who have undergone orthopaedic surgery will be accessed to see if they are meeting developed audit criteria based on the JBDS [19], NCPOD [21] and CPOC [23] guidance. |
| Audit duration | Data will be collected from healthcare records of individuals with diabetes who underwent an orthopaedic surgical procedure during October 2019 and March 2020. |
| Audit centres | UK based – secondary care setting |
| Aims and objectives | Aim To assess the level of compliance with regards to the NCPOD [21] and CPOC [23] guidance and plan appropriate interventions to improve care for individuals with diabetes who are undergoing a surgical procedure. Objectives To audit patient notes to assess compliance against audit criteria. To present audit results to stakeholders and plan interventions to support service improvement. Pilot planned interventions ready for implementation and re-audit. |
| Number of subjects | Approximately 50 records will be reviewed |
| Data analysis and collection | Approximately 50 medical records will be reviewed against the audit criteria. These will then be analysed to see if the recommended standards were met. |
Table 2: Audit protocol.
| Diagnosis and main inclusion criteria | Inclusion criteria Adults > 18 years Individuals with type 1 diabetes and type 2 diabetes controlled with oral or injectable therapy for diabetes management. Individuals who have undergone an orthopaedic surgical procedure which required fasting and an overnight admission (emergency or elective) Exclusion criteria Adults < 18 years old No diabetes or type 2 diabetes controlled by diet alone. Individuals who have undergone an orthopaedic surgical procedure which did not require fasting or an overnight admission (emergency or elective). |
Table 3: Inclusion and exclusion criteria.
The aim was to analyse the medical records of approximately 50 individuals who were undergoing an orthopaedic procedure. The inclusion and exclusion criteria helped to identify the individuals who were suitable to be included. During the time period chosen (October 2019 and March 2020), 166 individuals with diabetes underwent an orthopaedic procedure. Of these individuals, 78 met the inclusion criteria so were included within the audit.
Basic demographic data such as the individuals age and gender were included in the data collection so that these could aid with the data analysis. Only data relating to the ten audit criteria were collected in addition to the demographic data in order to comply with the data protection act [44].
The data found was compared to the current guidelines available and the standards identified. The data will be analysed and then presented in the form of bar graphs, scatter graphs and pie charts to allow for straightforward interpretation.
Results
The trust IT team were able to send the author a report with the names and hospital numbers of all individuals coded with having diabetes who underwent an orthopaedic procedure between 1st October 2019 and 31st March 2020. The data was sent in the form of an Excel spreadsheet which the author kept on a password protected USB stick.
The search identified166 individuals so the medical records of these individuals were analysed manually by the author.
From these, 78 met the inclusion criteria. For the 88 individuals excluded, two had their procedure carried out within a private hospital due to bed shortages which meant that their data was incomplete as it was recorded on a different IT system. 61 underwent day surgery which did not involve an overnight stay in hospital and 25 had diabetes but were not treated with any medications (Figure 1) (Table 4).
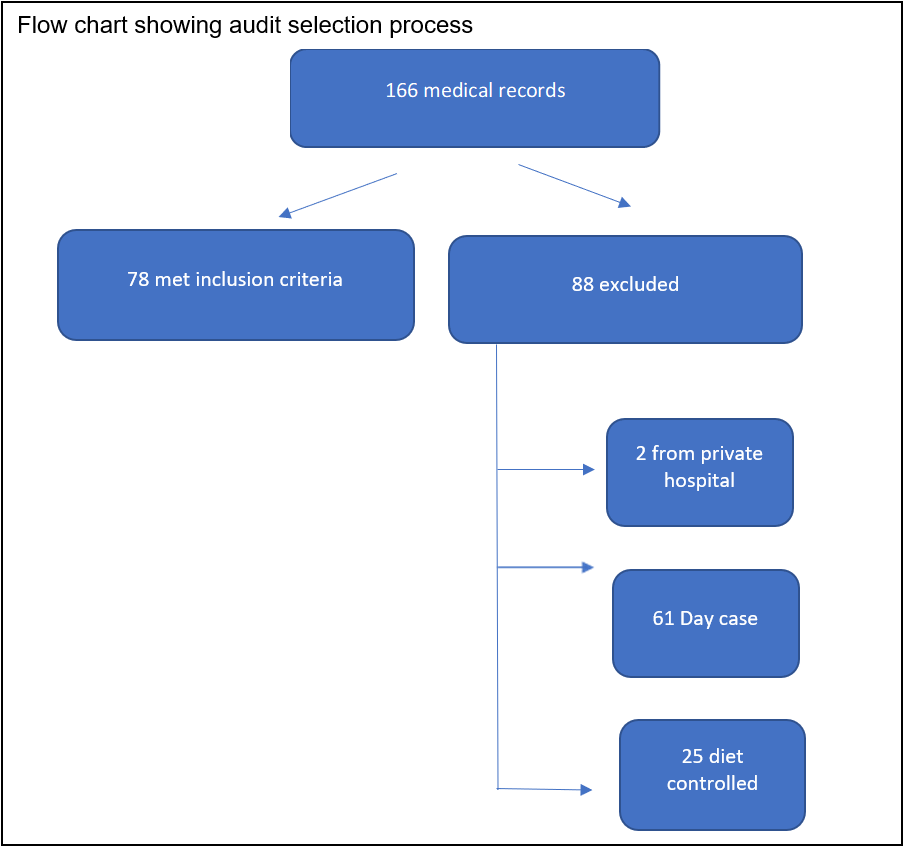
Figure 1: Flow chart showing audit selection process.
| Characteristic | Mean% |
| Age (years) | 71 (Male: 68; Female: 72) |
| Gender Male Female | 36% (28/78) 64% (50/78) |
| Diabetes type Type 1 Type 2 | 13% (10/78) 87% (68/78) |
| Surgical procedure Elective Emergency | 36% (28/78) 64% (50/78) |
Table 4: Characteristics of the audit population.
The age range of the individuals included in the audit was 30–91 years old, however the mean age was on the higher end of that scale at 71 (Figure 2).
There was a significant difference in the percentage of females to males, this may be due to the increased risk of osteoporosis in post-menopausal females which can lead to an increased risk of fractures.
The percentage of individuals with type 1 and 2 diabetes fits with the national prevalence of diabetes, with around 10% of all diabetes cases being type 1 compared to 90% being type 2.
The number of emergency cases were also considerably higher than the elective cases. This may have been due to the time of year that the audit was conducted as statistically, there are more slips and falls due to ice and cold weather in the winter months when the audit data was collected.
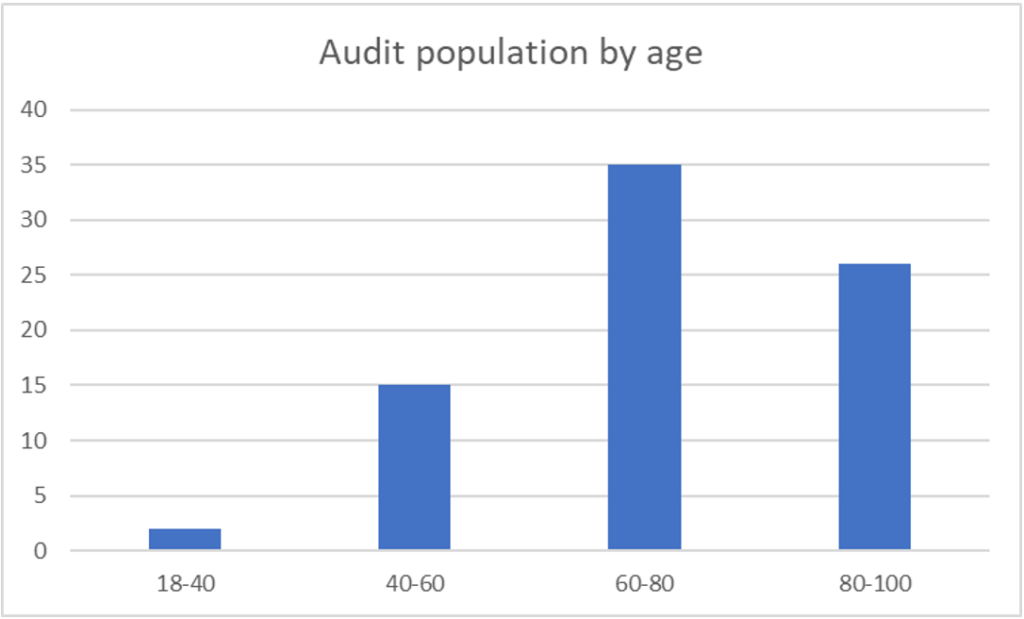
Figure 2: The age range of the audit population.
When broken down further, it is clear to see that the number of orthopaedic procedures that occur increased during older age (Figure 3).
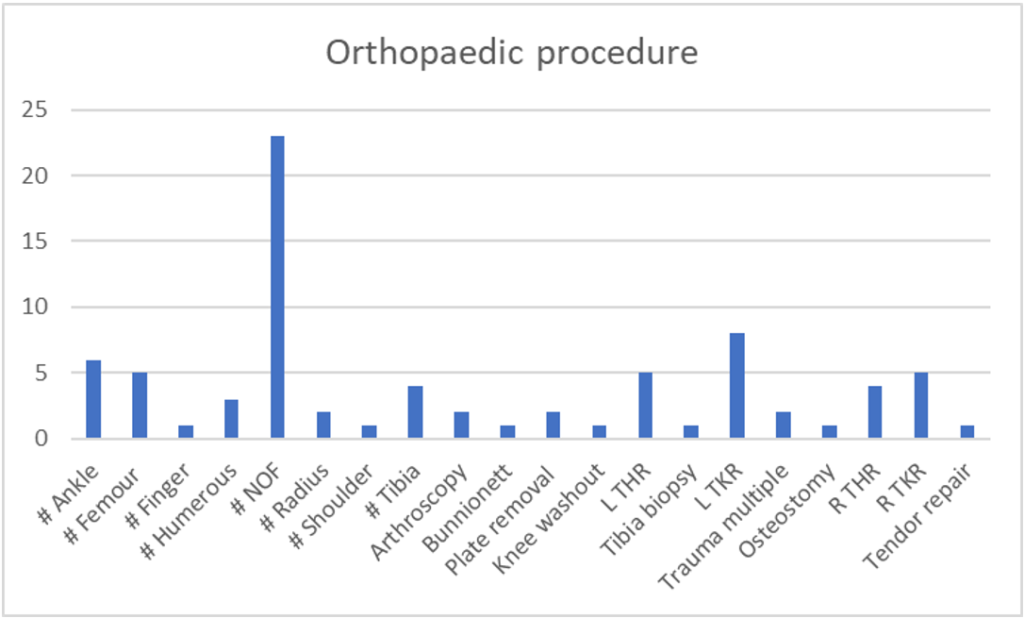
Figure 3: The orthopaedic procedures undertaken.
There were a variety of orthopaedic procedures that were carried out on individuals included within the audit. Knee and hip surgeries were by far the most common, either replacements or due to a fracture. This is also consistent with the age of individuals being operated on who were included within this audit. This data was collected to help describe the demographics of the population.
When the HbA1c levels of all the individuals included in the audit are compared, it is clear to see that they are quite varied. There were seven individuals where an HbA1c level was not available and are shown on the graph as zero. The most common reason for a missing HbA1c level was due to the individual being out of area so the author did not have access to their GP database. The missing HbA1c levels all occurred in individuals having emergency procedures. There is no real correlation between age and HbA1c as the youngest individual included in the audit had the highest HbA1c level where as one of the oldest individuals had the lowest HbA1c (Figure 4).
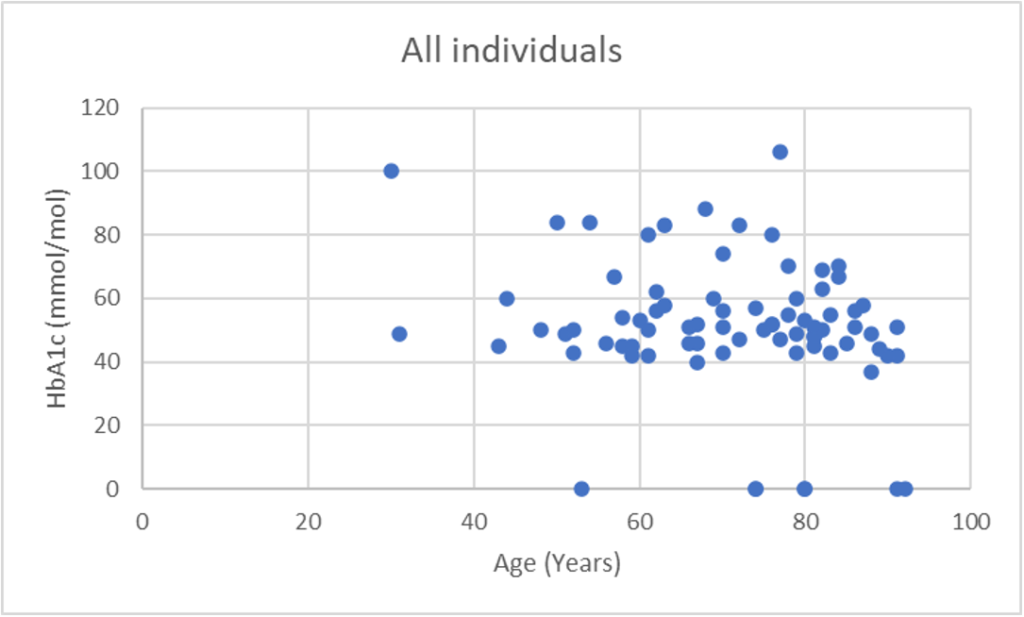
Figure 4: HbA1c of all the individuals included within the audit.
When analysing the HbA1c levels of the individuals who underwent an emergency procedure, there is a large range from 37–106 mmol/mol which had been taken within the past 6 months. Approximately a third of individuals who underwent an emergency procedure had an HbA1c level above the recommended 69 mmol/mol (Figure 5).
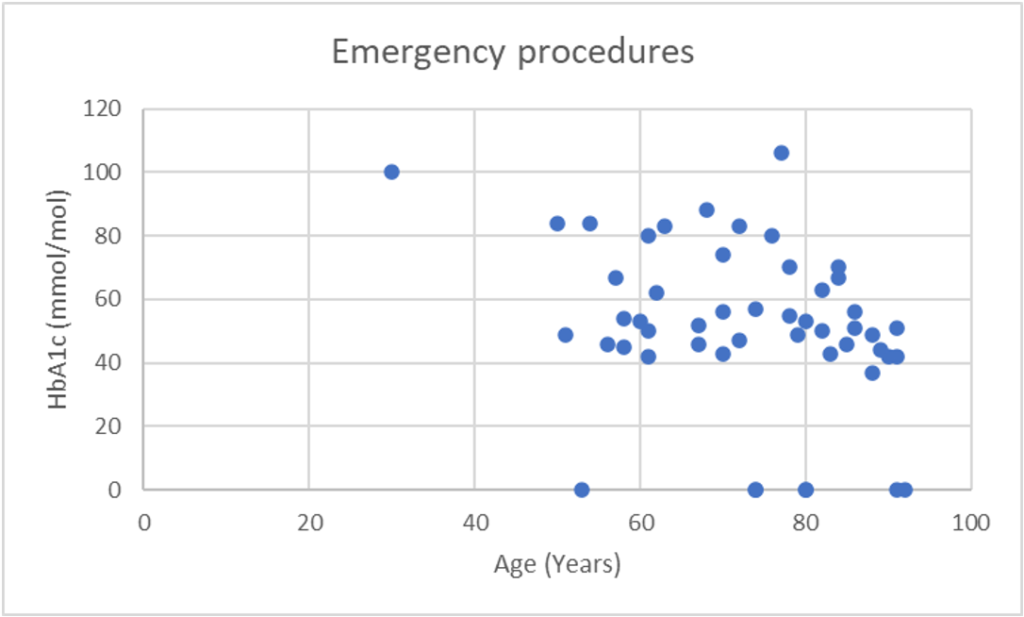
Figure 5: The HbA1c values of the individuals who underwent emergency procedures.
The HbA1c levels for individuals who underwent elective procedures were all under 69 mmol/mol, regardless of the individuals’ age. This would suggest that individuals are being appropriately screened within the pre assessment process to ensure that HbA1c levels are optimised prior to undergoing the surgical procedure (Figure 6).
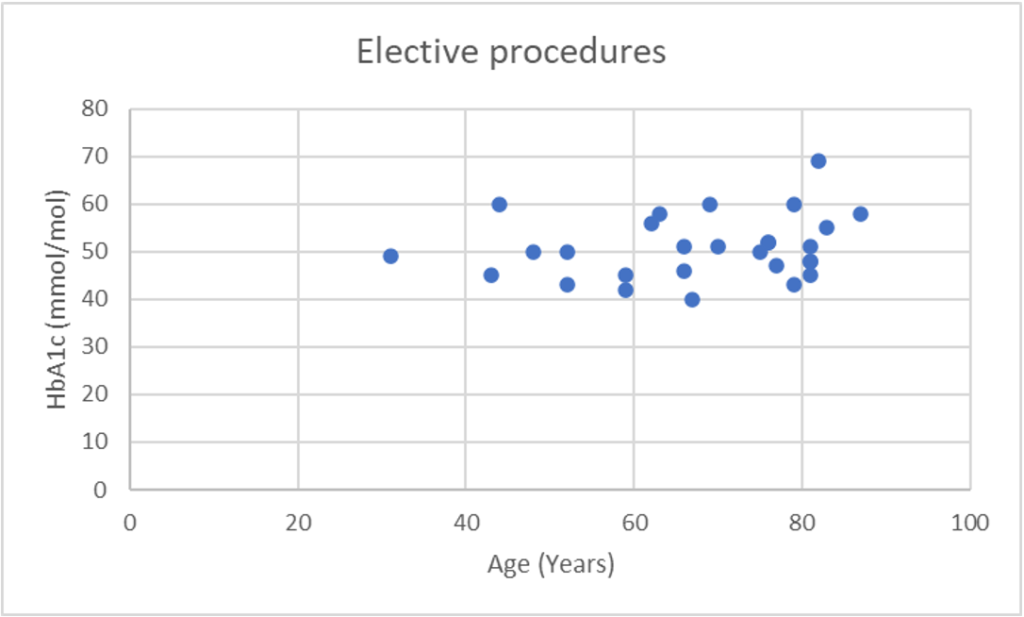
Figure 6: The HbA1c values of the individuals who underwent elective procedures.
Overall, the HbA1c levels were under 69 mmol/mol in over two thirds (66/78) of all individuals undergoing an orthopaedic procedure. This is a very reassuring number, however, shows that there is room for significant improvement.
The HbA1c levels were under 69 mmol/mol in 100% (28/28) of all elective procedure individuals. Within the emergency procedure individuals, the HbA1c was not available for 14% (7/50) of individuals and above 69 mmol/mol in 24% (12/50) of individuals. There was only one individual who was referred to the inpatient diabetes team on admission due to a new diagnosis of diabetes within the emergency procedure individuals. 22% (11/50) of the individuals undergoing an emergency procedure met the criteria for referral to the diabetes team pre procedure due to their elevated HbA1c however, this did not occur. Within the individuals who had an HbA1c > 69 mmol/mol, there was only one individual who was over 80 years of age and would have been classed as frail meaning their HbA1c level may have been acceptable in view of their comorbidities (Figure 7).
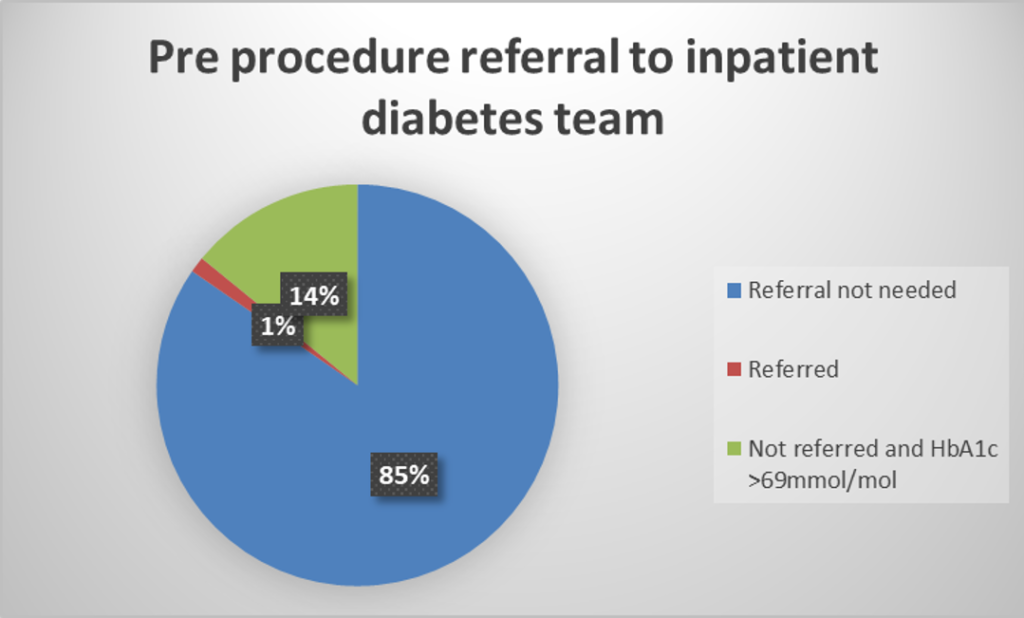
Figure 7: Individuals referred for diabetes specialist team review if HbA1c > 69 mmol/mol (elective and emergency).
Within individuals having an elective procedure, 82% (23/28) of individuals had their diabetes type recorded correctly. Whereas within the emergency procedure individuals, 90% (45/50) of individuals had their diabetes type recorded correctly. The incorrect documentations included some outdated terms such as IDDM and NIDDM, or the abbreviation DM. This occurred in five individuals within the elective procedure group as well as five individuals within the emergency procedure group. This is an area that needs to be focused on when providing education to the orthopaedic teams, explaining the reasons why it is so important to record the diabetes type accurately (Figure 8).
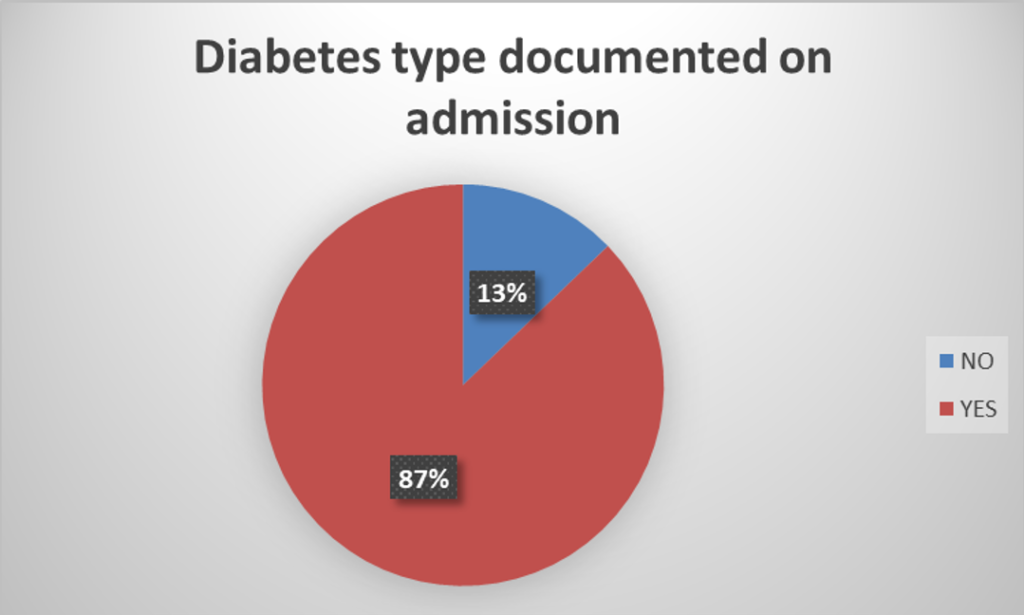
Figure 8: Diabetes type was documented on admission (elective and emergency).
A medicines reconciliation is a full list of medications that an individual is either prescribed or buys over the counter. This should include all oral, inhaled, injectable, topical and patches.
100% (28/28) of elective procedure individuals had an accurate medicines reconciliation completed on admission compared to 84% (42/50) of individuals who underwent an emergency procedure. All of the elective individuals underwent a pre-assessment clinic where the medications were clearly documented within their medical records. Within the individuals who did not have this completed accurately, the term ‘insulin’ was used, with the type of insulin not being specified. On one occasion, the documentation stated, ‘insulin four times a day’. This is something that the author has experienced first-hand on a number of occasions when reviewing the orthopaedic clerking of patients that are reviewed by the inpatient diabetes team. This is another example of an area that needs to be focused on when providing education to the orthopaedic teams (Figure 9).
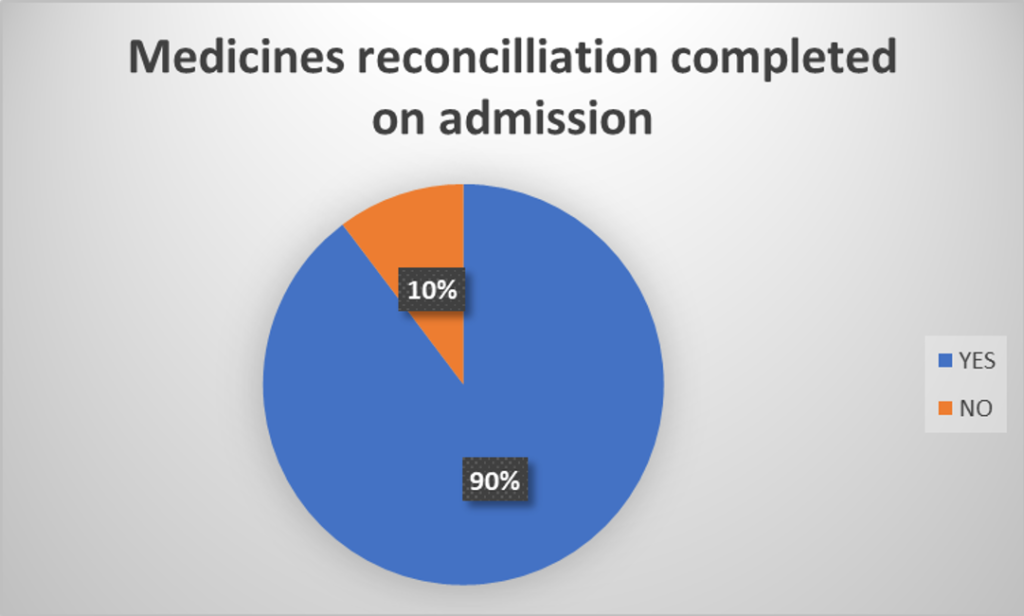
Figure 9: A medicines reconciliation was documented on admission (elective and emergency).
100% (28/28) of the elective procedure individuals had a medication plan made compared to 38% (19/50) of emergency procedure individuals. It was clear when reviewing the medical records to see how effective the pre assessment process was for the individuals undergoing elective procedures. The paperwork used within the pre assessment process clearly documented the medication review, formulating a pre and post procedure plan.
Within the emergency procedure individuals, there were twice as many individuals who were on oral therapy only who did not have a medication plan made compared to those on insulin. This is surprising as from the authors experience, there is often a great deal of clinical inertia by health care professionals surrounding the use and adjustment of insulin (Figure 10).
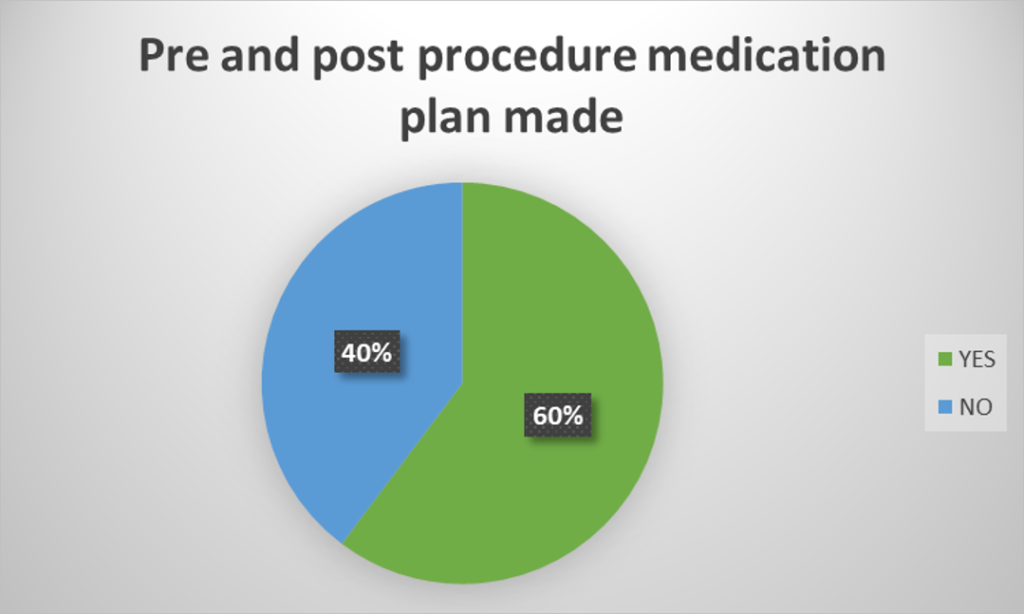
Figure 10: A medication plan was made for pre, during and post procedure (elective and emergency).
In the elective procedure individuals, 11% (3/28) had documentation to show that the time of surgery had been considered. This occurred in only 2% (1/50) of the emergency procedure individuals. This was unexpected as it was presumed that the number would have been higher in the elective procedure individuals due to the increased planning time available compared to the emergency procedures. Timing may have been considered by the surgical team but there was no standardised way of documenting this within the medical records. This is an area that could be improved going forward (Figure 11).
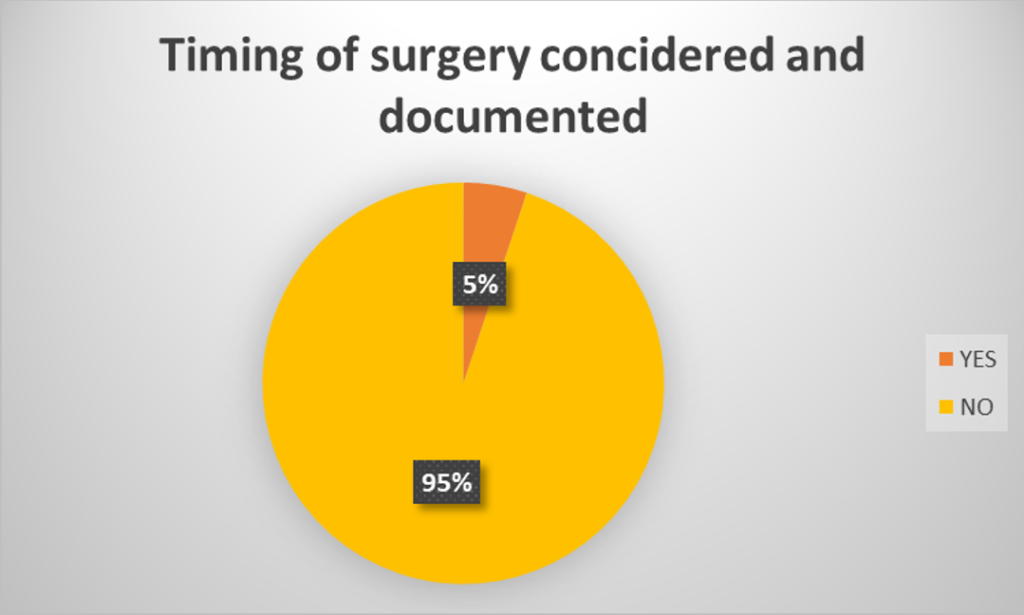
Figure 11: The timing of surgery was considered (e.g., prioritised to minimise fasting) (elective and emergency).
A VRIII was used in the elective procedure individuals in 7% (2/28) of cases. In the emergency procedure individuals this was much higher at 40% (20/50) of cases. Interesting, the low usage may be due to the time the surgery was performed as individuals with diabetes may have been prioritised to go to the top of the operating list even though there was no written confirmation of this decision-making process. There was no evidence in any severe hypoglycaemia in any of the individuals who were started on a VRIII. Within all the individuals who had type 1 diabetes, 80% (8/10) has a VRIII during their procedure. There was one individual who used an insulin pump and that was continued during the procedure, meaning that there was only one individual with type 1 diabetes included within the audit who did not have a VRIII started during their procedure (Figure 12).
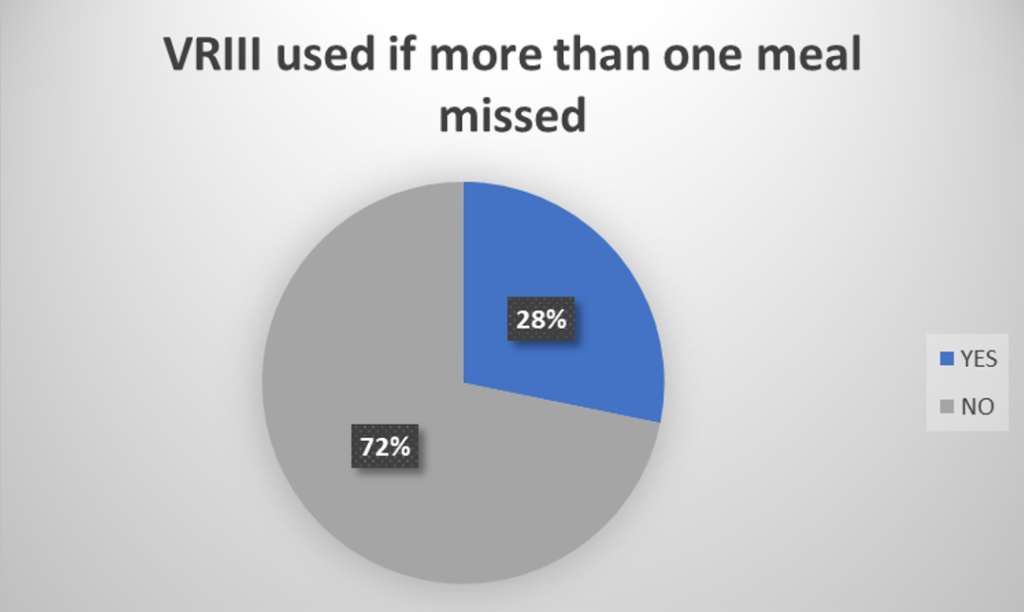
Figure 12: A VRIII was used if the patient was missing more than one meal (elective and emergency).
Individuals with type 1 diabetes receiving insulin at all times occurred 100% (2/2) of the time in the elective procedure individuals and 88% (7/8) of the time in emergency procedure individuals. From the data available, it does not appear that any individual came to harm due to this, however there is evidence of hyperglycaemia for short periods of time (Figure 13).
Within the elective procedure individuals, 79% (22/28) achieved blood glucose levels (BGLs) between 6–12 mmol during their entire admission compared to 44% (22/50) of emergency procedure individuals. For both the elective and emergency procedure individuals, the individuals who were usually on insulin were 50% (39/78) more likely to have hyperglycaemia during their admission compared to those on oral agents. Age was also a factor to consider. Within the elective procedure individuals, 68% (19/28) of those who were hyperglycaemic were over the age of 70. In the emergency procedure individuals, 36% (18/50) were over the age of 70. It is clear from these results that hyperglycaemia post procedure is common and further education for the surgical and ward teams of the management of hyperglycaemia is required (Figure 14).
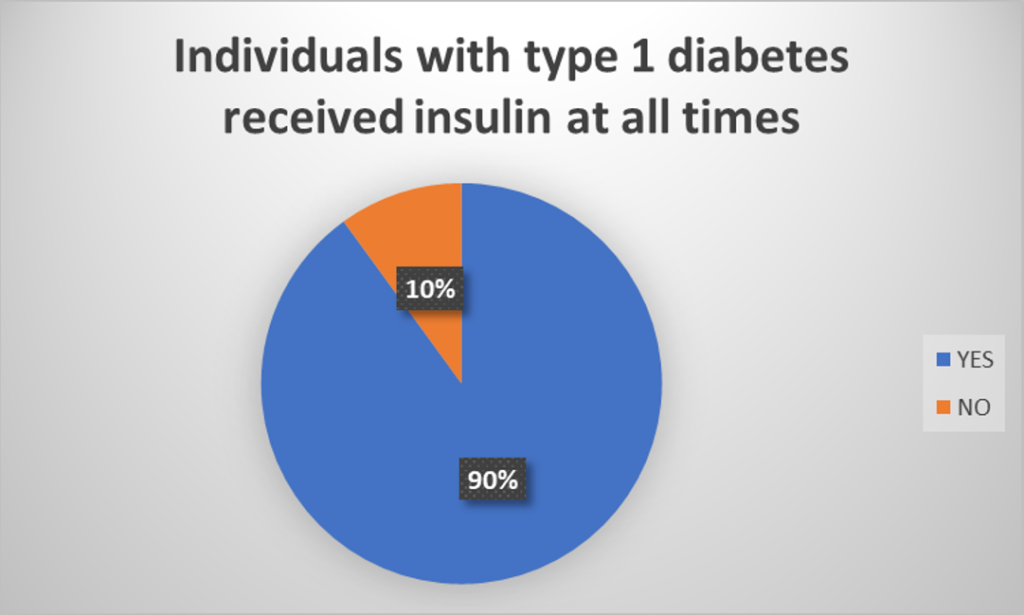
Figure 13: Individuals with type 1 diabetes received insulin at all times (elective and emergency).

Figure 14: Blood glucose levels were maintained between 6–12 mmol/l during the admission (elective and emergency).
Within the elective procedure individuals, 50% (3/6) had blood ketone levels monitored if appropriate compared to 68% (15/22) of emergency procedure individuals. Further education is required on the indications when to monitor blood ketone levels (Figure 15).
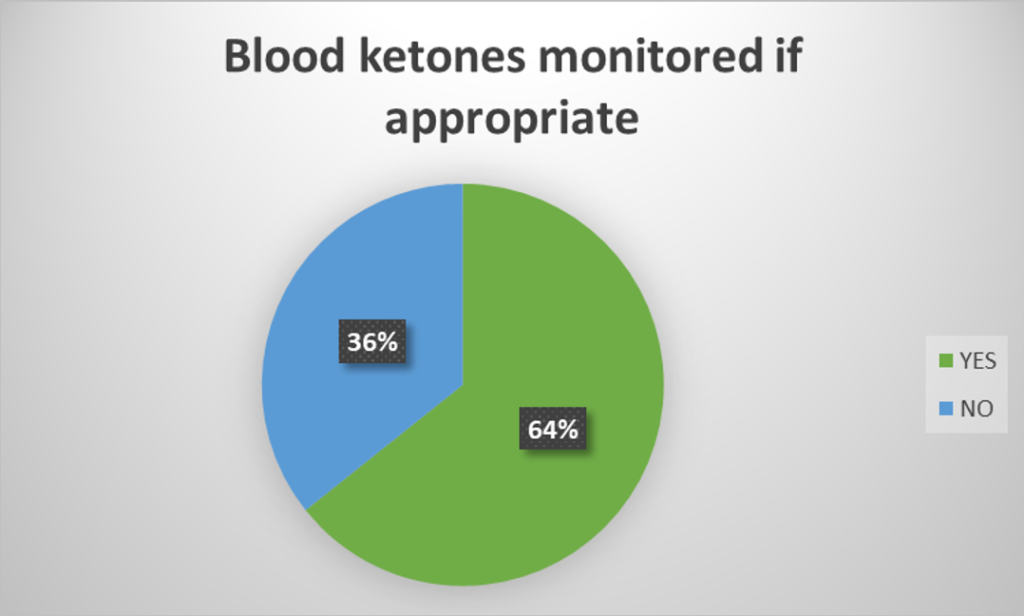
Figure 15: Ketone levels were monitored if indication (e.g., type 1 diabetes or significant hyperglycaemia) (elective and emergency).
Just under two thirds (57/78) of individuals did not require a referral to the inpatient diabetes team based on the referral criteria. Within the elective procedure individuals, 7% (2/28) needed a referral to the inpatient diabetes team and this occurred in 100% (2/2) of cases. Within the emergency procedure individuals however, 38% (19/50) of individuals required a referral, and this occurred in 32% (6/19) of cases meaning that 3 individuals who needed to be seen by the inpatient diabetes team did not get referred. The referral criteria used was based on the trust’s inpatient diabetes referral tool (Figure 16) (Appendix 2).
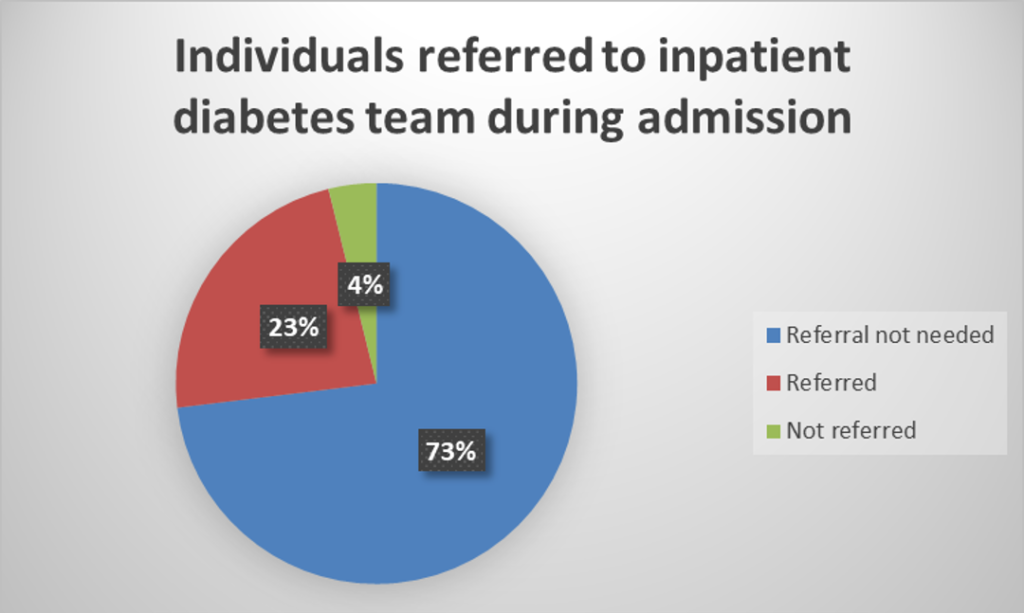
Figure 16: Individuals were referred to the inpatient diabetes specialist team according to their criteria (elective and emergency).
Key findings
The audit has produced some interesting results within individuals undergoing both elective and emergency orthopaedic procedures.
The audit participants were in their later stages of life with the mean age being 71 years of age. There was a large proportion of females included in the audit, equating to nearly two thirds of the audit population. It was felt that this was due to the increased risk of osteoporosis in post-menopausal women which can lead to an increase fracture risk.
87% (68/78) of the audit participants had type 2 diabetes compared to 13% (10/78) with type 1 diabetes. This is the approximate figure expected as it is in line with the national prevalence of both type 1 and 2 diabetes.
There was an unexpected split of elective and emergency procedures, with nearly two thirds of the procedures being emergency. The audit data was collected retrospectively from procedures that occurred between 1st October 2019 and 31st March 2020 which may have influenced the increased number of emergency procedures due to falling within the winter months.
There were a variety of procedures that were undertaken during this period but the most common were highlighted to be hip and knee surgery.
All the participants undergoing elective procedures has an HbA1c below 69 mmol/mol, but the author did not investigate whether they had been rescheduled due to a previously higher HbA1c. Within the individuals undergoing emergency surgery, two thirds had an HbA1c under 69 mmol/mol which was encouraging to see.
When reviewing the data for the ten audit criteria, there were some significant differences between individuals who had undergone elective and emergency procedures. When reviewing whether individuals had an HbA1c < 69 mmol/mol pre surgery, it was pleasing to see that 100% (28/28) of individuals undergoing elective surgery had an HbA1c < 69 mmol/mol. Within the emergency procedure individuals, the large majority had an HbA1c < 69 mmol/mol however 14% (7/50) of individuals may have benefited from a review to the diabetes team as they had an Hba1c > 69 mmol/mol and were not referred. The author did not investigate however whether the individuals had previously been reviewed by a diabetes specialist prior to the pre assessment process.
Correctly documenting the type of diabetes is extremely important for ongoing management of an individual. A large percentage, 87% (68/78) of individuals had their correct diabetes type documented within their medical records however, 13% (10/78) had inaccurate documentation or outdated terminology which can be misleading. There were similar rates of documentation within the elective and emergency procedure groups, with 82% (23/28) and 90% (45/50) respectively having the correct diabetes type documented in their medical records.
An accurate medicine reconciliation is vital for all individuals in hospital. This was seen to have been carried out in 90% (70/78) of individuals prior to their procedure. Within the elective procedure individuals, 100% (28/28) had their medications accurately documented within their medical record. This was completed in a structured manner using a template within the pre assessment documentation. Within the emergency procedure individuals, 84% (42/50) had an accurate medication reconciliation however, this may account for some individuals who were amidst to hospital and having their procedure within hours of admission, reducing the amount of time for an accurate assessment. These patients may have also been in pain or been involved in a traumatic incident thereby reducing their ability to provide an accurate list of medications prior to their procedure.
A plan with regards to medication pre, during and post procedure is essential in the management of these individuals. A medication plan was only documented in 60% (47/78) of individuals, clearly showing an area that requires improvement. This was completed however, in 100% (28/28) of elective procedure individuals, again showing how effective the use of a pre assessment appointment is. Only 38% (19/28) of emergency procedure individuals had a documented medication plan. This is an area that requires further improvement with possibly an ‘emergency pre assessment’ form being created to document these plans.
The documentation of the planned timing of a procedure was poor within both elective and emergency cases. Only 5% (4/78) of individuals had written documentation to highlight the need to prioritise the individual due to their diagnosis of diabetes. That being said, the majority of patients (especially elective individuals) were operated on in the morning slots so maybe the decision was made to prioritise but just not documented within the medical notes. Unsurprisingly, only 2% (1/50) of emergency procedure individuals had documentation to state that they should be prioritised to the morning list to minimise the time of fasting. These individuals may have needed immediate surgery so this would not have been possible. Unexpectedly however, only 11% (3/28) of elective patient had documentation to prioritise them to the morning lists. The author would have envisaged this a much higher number would have had this documented within their medical records.
The use of a VRIII during the procedure was much more common in individuals undergoing an emergency procedure (40% or 20/50) than an elective one (7% or 2/28). This may have been due to the emergency procedure individuals being in state of acute illness, and stress, causing hyperglycaemia on admission. 90% (9/10) of individuals with type 1 diabetes received insulin at all times during their admission. The individuals who missed insulin on at least one occasion were all undergoing emergency procedure. 100% (28/28) of the elective procedure individuals received insulin at all times during their admission. The medication plan that was formulated within the pre assessment period may have been one of the reasons for this.
The monitoring of blood glucose levels was generally carried out adequately on all of the individuals within the audit group. Maintaining a level between 6–12 mmol/l however, only occurred in just over half of individuals (56% or 44/78). Predictably, the individuals undergoing elective procedures were more likely to have blood glucose levels within range compared to the individuals undergoing emergency procedures. This occurred in 79% (22/28) of individuals and again may be due to the comprehensive medication plan that was made during pre-assessment.
The monitoring of blood ketone levels is generally recommended within type 1 diabetes and in type 2 diabetes during times of acute illness and or hyperglycaemia. Ketone monitoring occurred in 64% (18/28) of individuals who met the criteria for carrying this out. There were slightly more ketone tests carried out within emergency procedure individuals (68% or 15/22) compared to the individuals undergoing elective procedures (50% 3/6). This may have been due to the clinical condition of the individuals who were admitted acutely and required a surgical procedure as they were more likely to have hyperglycaemia on admission to hospital.
During an individual’s admission, it is not uncommon for an individual to require referral to the inpatient diabetes team to help stabilise their blood glucose levels. Around a quarter of individuals were referred to the inpatient diabetes team, however, a further 4% (3/78) of individuals met the criteria for a referral but this was not made. 100% (2/2) of elective procedure individuals were referred to the diabetes team appropriately if they met the criteria for referral. 38% (19/50) of emergency procedure individuals required a referral to the diabetes team, 84% (16/19) had a referral sent.
Suggestions
Individuals with diabetes should be referred to diabetes specialist team if their HbA1c is > 69 mmol/mol pre procedure
All staff involved in the pre assessment of emergency and elective patients need to undergo education to reiterate the need for a referral to the diabetes specialist team if an individual has an HbA1c > 69 mmol/mol. This seems to be engrained into the pre assessment staff who are dealing with elective patients; however, it is important to stress the need for emergency patients to also be referred, so that their medications can be optimised in order to improve post operative wound healing. Access to the online diabetes team referral form needs to be promoted to all surgical staff. In order to practically achieve this, it was agreed within the stakeholder meetings that an education session would be delivered by the diabetes team. This session would be recorded so that staff unable to attend can watch at a time that suits them. The diabetes team have also offered healthcare professionals within orthopaedics the opportunity to spend time with them on their diabetes ward rounds.
The type of diabetes should be documented in the medical record, particularly on the anaesthetic record
Education is also required for junior surgical doctors and advanced nurse practitioners (who undertake the majority of the clerking) regarding the appropriate terminology that should be used when documenting the type of diabetes an individual has. This should also include where this should be documented and the importance of this.
A medicines reconciliation is carried out on admission to hospital and written in the medical record
It was clear that the pre-assessment paperwork used within the elective patients was very effective. The author would like to develop a similar emergency ‘pre-assessment’ form that can be used to ensure all the documentation is correct and checked pre procedure (similar to the one used for elective procedures). This could be trialled for a short period of time and then feedback sought from the surgical teams.
A medication plan to be made for pre, during and post procedure
The author feels that a written plan could be included on the emergency ‘pre assessment’ form so that the ward nurses have some guidance with regards to the medications that need to be held. It is important that these are also prescribed on the electronic prescribing system used within the author’s trust. Education on how to do this can be included within the education session that will be held.
Timing of surgery considered
This documentation would be ideally included within the elective and emergency pre assessment forms. The author suspects that a number of individuals included in the audit did have their procedure time considered but there is no specific place currently for this to be documented. The re-audit will be beneficial to review the effect this has had on patient care.
A VRIII is used if missing more than one meal
Documentation of whether a VRIII is required, could also be included on the pre assessment form so that the ward staff are aware well in advance if they need to start a VRIII. This will also help to guide whether an individual requires admission the day prior to the procedure. Again, the results of the re-audit can be analysed to see if this has brought about improvements within this area.
Individuals with type 1 diabetes receive insulin at all times
It is important that staff are educated with regards to the need for insulin to be documented in the medical records and that it is accurately prescribed and administered. If a medication plan was documented, this would reduce the likelihood of insulin being missed. Education regarding the types of diabetes and the differences between these will be included in the proposed education session.
Maintaining blood glucose levels between 6–12 mmol/l during admission
The frequency of blood glucose monitoring could be documented on the pre assessment form. This could vary depending on the type of diabetes an individual has as well as the medication that they are taking. Ward staff need to be reminded of the need to refer individuals to the inpatient diabetes team (using the electronic referral form) if the levels are out of range after the surgical team have made any changes to medication doses. The education session planned will cover this.
Ensuring ketone levels are monitored if indicated
Further education is required and will be covered in the planned education session for surgical juniors and nursing staff regarding the appropriate indications to monitor ketone levels. The blood glucose at which an individual requires blood ketone monitoring could also be included on the pre assessment form.
Individuals are referred to the inpatient diabetes team during their admission if they meet criteria
The surgical juniors and nursing staff need to be reminded of the need to refer individuals to the inpatient diabetes team (using the electronic referral form) if blood glucose levels are out of range after surgical team intervention. A discussion on how to refer to the diabetes team and in particular, who to refer will be covered within the education session.
The main intervention that the author plans to undertake on the back of this audit is the pilot of a pre-assessment form for individuals undergoing emergency surgery. By having an additional form for these individuals, it is anticipated that the audit criteria adherence will improve if this was re-audited.
The author plans to pilot the use of this form within one of the orthopaedic surgical wards and obtain feedback from the surgical nursing and medical staff in its ease of use and effectiveness.
Providing an education session for the health care professionals working within orthopaedics is a further intervention that will aim to enhance the care received by individuals with diabetes who are undergoing an orthopaedic procedure. This is something that can be repeated again within a few months to ensure new staff have access to this clinical update. During this session, the importance of documentation is an area that also needs to be discussed, especially if the new form is to be piloted within orthopaedics.
A re-audit can then be undertaken to see if the standard of care has improved for individuals with diabetes who are undergoing an orthopaedic procedure.
Conclusion
The audit showed that whilst the majority of individuals with diabetes undergoing an orthopaedic procedure at the authors trust received a satisfactory standard of care, however, there were a few areas that could be improved.
Clinical audit is a quality improvement process which aims to improve patient care and patient outcomes by comparing the care received by individuals against explicit criteria and the implementation of change [45]. Therefore, clinical audit was used as a methodology to compare the standards of care received by individuals with diabetes who were undergoing orthopaedic procedures against the current national guidance.
The audit found that all individuals undergoing an elective procedure (100%) had an HbA1c of < 69 mmol/mol. Within the individuals undergoing emergency procedures however, only 69% had an HbA1c < 69 mmol/mol. The fact that individuals undergoing elective procedures had an HbA1c below the target range is not surprising as there was time to intensify the individual’s treatment prior to the procedure. This would not have been possible due to the urgent nature of individuals undergoing emergency procedures.
The correct documentation of an individual’s diabetes type was generally completed correctly in most individuals.
A medicines reconciliation and post procedure plan were completed in all individuals undergoing elective surgery whereas, there is clear evidence for improvement for individuals undergoing emergency procedures, particularly in documenting the post procedure plan.
Very low number of individuals had the fact that the timing of their procedures had been considered documented (2–11%).
The usage of a VRIII was low (7%) in elective procedures, possibly because all individuals had a medication plan made. More individuals (40%) had a VRIII initiated if they were undergoing emergency procedures. This is to be expected as individuals may have other factors affecting their blood glucose control due to their unplanned admission.
All individuals with type 1 diabetes (100%) always received insulin if they were undergoing elective procedures compared to 88% of those who underwent an emergency procedure.
Blood glucose levels were maintained between 6–12 mmol/l in less than half (44%) of individuals undergoing emergency surgery whereas 79% achieved these levels if they underwent elective procedures. Half of the individuals (50%) undergoing elective procedures appropriately had their blood ketone levels monitored compared to 68% of individuals who underwent an emergency procedure.
Referrals to the inpatient diabetes team were completed for all those that required one if they underwent elective procedures, however only 32% of individuals who required a referral were referred if they underwent an emergency procedure.
Age
The individuals undergoing an orthopaedic procedure requiring an overnight admission had a mean age of 71 years. This may have influenced the audit due to the coexisting comorbidities that this group of individuals may also have had. They are statistically more likely to have had a longer duration of diabetes due to their age.
Gender
Two thirds of the audit population were female, this may have been due to the increased risk of osteoporosis in the post-menopausal population leading to an increased risk in fractures.
Diabetes type
The percentage of individuals with type 1 and type 2 diabetes were consistent to that expected within the general population.
Emergency vs elective procedures
The audit data was collected retrospectively, prior to Covid-19, in order to minimise the risk of bias towards elective procedures as it was felt that there would have been several elective procedures that would have been cancelled during this period. Even by doing this, two thirds of the procedures were emergency compared to elective.
With the exception of the documentation of diabetes type, use of VRIII and monitoring of blood ketones, the individuals undergoing elective procedures received a higher standard of care within the audit criteria measured.
Comparison of audit findings with existing evidence
The JBDS [19] and NCPOD [21] guidance are more focused on elective procedures whereas the CPOC [23] suggests guidance for both elective and emergency surgery. The audit carried out by the author compares the standards proposed within these guidelines to see how this differs between elective and emergency admissions.
The optimal pre-operative HbA1c level has been debated for several years, with a consensus now agreeing on a value of < 69 mmol/mol [6]. This was shown to be advantageous, certainly within the individuals undergoing elective procedures as overall, they were much more likely to have blood glucose levels within the suggested target of 6–12 mmol/l.
The period of hyperglycaemia caused by a stress response along with the period of starvation pre procedure can be responsible for individuals to have blood glucose levels outside of the target range of 6–12 mmol/l [33]. This was seen particularly within individuals undergoing emergency procedures. Steroid injections are also frequently used for a range of orthopaedic conditions which can further cause hyperglycaemia in individuals with diabetes [33]. The use of steroid was not investigated within this audit.
The audit showed that there were differences in the standards or care received by individuals undergoing elective and emergency procedures. Negus et al. [33] state that this is expected due to the period of planning that can be undertaken with individuals undergoing elective procedures compared to a much shorter duration of time (sometimes hours) with individuals undergoing emergency procedures. It is well documented however, that individuals with diabetes are more likely to require emergency orthopaedic procedures for a number of reasons such as, hypoglycaemia, causing an increased risk of falls and a reduced bone density, increasing the fracture risk [31]. This may account why the number of individuals undergoing emergency procedures was considerably higher than the elective procedures within the audit.
Within their systematic review, Wallace et al. [16] showed similar outcomes to this audit where individuals undergoing elective procedures had a slightly more advantageous outcomes compared to those undergoing emergency procedures.
National guidance suggests that individuals with diabetes should be listed first on the operating lists [33], this audit shows that there needs to be a more effective way that this decision is documented within the medical records as there was little evidence that this occurred.
Negus et al. [33] suggest that appropriate medications for perioperative hypoglycaemia and hyperglycaemia should be prescribed in advance of surgery, this was not always the case, as shown in the audit, particularly with individuals undergoing emergency procedures. Franco et al. [29] suggest using an algorithm which can direct health care professionals in how to adjust medications in the days leading up to surgery. The pre assessment form used for individuals undergoing elective surgery prompted a plan to be made. Therefore, the author feels a similar form is required for individuals undergoing emergency procedures in an attempt to ensure medication plans are made.
Encouraging individuals to self-manage their diabetes is extremely important [30]. This was an area that was not investigated within this audit as it may have influenced the ability to achieve blood glucose levels between 6–12 mmol/l.
Insulin is generally the recommended method to achieve adequate glycaemic control within the hospital setting [32]. VRIII are commonly used, however this was not the case within this audit which is possibly a reason why the individuals who underwent emergency procedures only had blood glucose levels between 6–12 mmol in 44% of cases. VRIII are however, associated with a number of complications so it is important that guidelines are available to ensure they are used safely [4].
Early involvement of the diabetes team is suggested, especially in the case of emergency admissions [3]. With this in mind, it was a little disappointing to see that only 32% of individuals who underwent emergency procedures that required referral to the diabetes team had a referral sent. This figure is significantly higher than shown by Diabetes UK within their ‘Making hospitals safe for people with diabetes’ publication where it was suggested that 28% of individuals who needed a review by the specialist diabetes team in hospital did not get referred [39].
Within the guidelines, there is a focus on ‘general’ surgery whereas the author has focused specifically on the field of orthopaedic procedures. This is an area where there has been limited research conducted previously.
Within the audit, age was shown to be a significant variable that needed to be taken into consideration whereas this was not mentioned in detail within the three main guidelines.
There were some significant differences within the care received by individuals undergoing emergency procedures rather than elective. This is an area that also needs more investigation to ensure parity in care can be provided. Levy et al. [4] agree stating that there have been much published regarding improving the outcome of individuals with diabetes who undergo elective surgical procedures whereas individuals undergoing emergency procedures have been largely ignored.
One of the strengths of the audit was the focus area. Individuals undergoing orthopaedic procedures is an area that is lacking in research. Individuals with diabetes who undergo orthopaedic surgery have a risk of infection, more than double that of individuals without diabetes [33]. Diabetes significantly increases mortality risk after total hip replacement and individuals with diabetes are also known to suffer from chronic musculoskeletal conditions [34].
Being able to compare both emergency and elective procedures, also enabled the author to review both admission pathways and highlight some significant differences. The main limitation of the audit was the size. A population of 78 is relatively small and there was a disproportionate number of individuals undergoing emergency procedures compared to elective procedures. The time of year may have had an influence on the results as this was undertaken within the autumn and winter months, typically where there is an increase in falls within the older population.
A further limitation is that the author did not investigate whether any of the individuals undergoing elective procedures had been rescheduled due to a previously higher HbA1c.
Diabetes teams often have a lower threshold for discharging individuals with diabetes and can considerably reduce the LOS of an individual [31]. LOS is also found to be significantly longer in individuals undergoing emergency procedures than those undergoing elective ones [16].
The duration of stay was not evaluated within this audit to see whether it differed between elective and emergency procedures or if it was reduced if the inpatient diabetes team had reviewed the individual.
National guidance with regards to individuals with diabetes undergoing surgical procedures have been available since 2011 [19]. It is clear however, from this audit, that there are differences in the care received by individuals undergoing emergency and elective procedures which needs to be considered.
The CPOC [23] guidance has highlighted the need for guidance for both elective and emergency procedures more recently, with their guidance covering both areas. There is also evidence that there are some differences in the care required by individuals with diabetes who are undergoing an orthopaedic procedure rather than ‘general surgery’. It may be the case that separate surgical guidelines are required for different specialities, such as orthopaedics.
Within the audit, age was a factor that the author was not expecting to be an issue. With the mean age being 71, it is clear that further guidelines need to consider this as care may need to be adapted. The older age group may be due to the speciality of the procedures investigated, so further research into orthopaedic procedures in particular is required.
Supplementary Material
References
- Diabetes UK. New stats people living with diabetes. 2019.
- NHS Digital. National Diabetes Inpatient Audit England and Wales. 2018.
- Dhatariya K, Levy N, Kilvert A, et al. NHS Diabetes guideline for the perioperative management of the adult patient with diabetes. Diabet Med. 2012;29(4):420-33.
- Levy N, Penfold NW, Dhatariya K. Perioperative management of the patient with diabetes requiring emergency surgery. BJA Education. 2016;17(4):129-136.
- Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85(1):109-17.
- Barker P, Creasey PE, Dhatariya K, et al. Peri-operative management of the surgical patient with diabetes 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2015;70(12):1427-40.
- Partridge H, Perkins B, Mathieu S, et al. Clinical recommendations in the management of the patient with type 1 diabetes on insulin pump therapy in the perioperative period: a primer for the anaesthetist. Br J Anaesth. 2016;116(1):18-26.
- Fletcher E, Askari A, Yang Y, et al. Diabetes in day case general and vascular surgery: A multicentre regional audit. Int J Clin Pract. 2020;74(4):e13472.
- Garg R, Schuman B, Bader A, et al. Effect of Preoperative Diabetes Management on Glycemic Control and Clinical Outcomes After Elective Surgery. Ann Surg. 2018;267(5):858-862.
- Moghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009;32(6):1119-31.
- UK Prospective Diabetes Study (UKPDS) Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853.
- Griesdale DE, de Souza RJ, van Dam RM, et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ. 2009;180(8):821-7.
- Kerr M. Inpatient Care for People with Diabetes: The Economic Case for Change. 2011.
- Dhatariya K, Levy N. Perioperative diabetes care. Clin Med(Lond). 2019;19(6):437-440.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care. 2010;33(8):1783-8.
- Wallace J, Jiwani SI, Gyasi-Antwi P, et al. Management of diabetes patients across the peri-operative pathway: A systematic review. Endocrinol Diab Metabol. 2020;4(1):1-16.
- Association of Surgeons of Great Britain and Ireland. Issues in professional practice: Guidelines for implementation of enhanced recovery protocols. 2009.
- Association of Anaesthetists of Great Britain and Ireland. Peri‐operative management of the surgical patient with diabetes 2015. Anaesthesia. 2015;70(12):1427-1440.
- Joint British Diabetes Society (JBDS). Management of adults with diabetes undergoing surgery and elective procedures: improving standards. 2011.
- Lipp A. Managing Diabetes in Patients Having Day and Short Stay Surgery. 4th ed. Bads Handbooks: British Association of Day surgery; 2016.
- Highs and Lows: A review of the quality of care provided to patients over the age of 16 who had diabetes and underwent a surgical procedure. 2018.
- McCavert M, Mone F, Dooher M, et al. Peri-operative blood glucose management in general surgery – a potential element for improved diabetic patient outcomes – an observational cohort study. Int J Surg. 2010;8(6):494-8.
- Centre for Perioperative Care (CPOC). Guideline for Perioperative Care for People with Diabetes Mellitus Undergoing Elective and Emergency Surgery. 2021.
- Rayman G, Kar P. Diabetes GIRFT Programme National Specialty Report. 2020.
- Johnston P, Newland-Jones P. Insulin self-administration: Development of an assessment tool to empower hospital in patients with diabetes. J Diab Nursing. 2017;21(5):174-178.
- NHS England. Never Events list 2018 First published January 2018. 2021.
- Department of Health. National service framework for diabetes: Care of people with diabetes during admission to hospital. 2007.
- Flanagan D, Moore E, Baker S, et al. Diabetes care in hospital–the impact of a dedicated inpatient care team. Diabet Med. 2008;25(2):147-51.
- Franco T, Rupp S, Williams B, et al. Effectiveness of standardised preoperative assessment and patient instructions on admission blood glucose for patients with diabetes undergoing orthopaedic surgery at a tertiary referral hospital. BMJ Open Qual. 2019;8(2): e000455.
- Hommel I, van Gurp PJ, Tack CJ, et al. Perioperative diabetes care: room for improving the person centredness. Diabet Med. 2015;32(4):561-8.
- Akiboye F, Rayman G. Management of Hyperglycemia and Diabetes in Orthopedic Surgery. Curr Diab Rep. 2017;17(2):13-23.
- Wukich DK. Diabetes and its negative impact on outcomes in orthopaedic surgery. World J Orthop. 2015;6(3):331-339.
- Negus OJ, Watts D, Loveday DT. Diabetes: a major risk factor in trauma and orthopaedic surgery. Br J Hosp Med. 2021;82(1):1-5.
- Rizvi AA, Chillag SA, Chillag KJ. Perioperative management of diabetes and hyperglycemia in patients undergoing orthopaedic surgery. J Am Acad Orthop Surg. 2010;18(7):426-35.
- Underwood P, Askari R, Hurwitz S, et al. Preoperative A1C and Clinical Outcomes in Patients with Diabetes Undergoing Major Noncardiac Surgical Procedures. Diabetes Care. 2014;37 (3):611-6.
- Reich MS, Fenandez I, Mishra A, et al. Diabetic control predicts surgical site infection risk in orthopaedic trauma patients. J Orthop Trauma. 2019;33(10):514-517.
- Page E, Allen R, Wensley F, et al. Improving the peri-operative pathway of people with diabetes undergoing elective surgery: the IP3D project. Diabet Med. 2020;37(12):2019-2026.
- Department of Health. Never events list 2018. 2021.
- Diabetes UK. Making hospitals safe for people with diabetes. 2018.
- Shankar AN, Shankar VN, Praveen V. The Basics in Research Methodology: The Clinical Audit. J Clin Diagnostic Res. 2011;5(3):679-682.
- Healthcare Quality Improvement Partnership. 2021.
- National Diabetes Inpatient Audit (NADIA). 2019 Audit. 2019.
- Department of Health. The Caldicott Committee Report on the Review of Patient-Identifiable Information. 1997.
- Data Protection Act. Data Protection Act 2018. 2018.
- National Institute for Health and Clinical Excellence. Principles of best practice in clinical audit. Oxford: Radcliffe Medical Press. 2002.
