Madnoorkar N *1, Vanere V2, Raina A3 and Madnoorkar S4
*1, Vanere V2, Raina A3 and Madnoorkar S4
1Surgical Oncology, Vasundhara Cancer Clinic, Nashik, India
2Histopathology, Agilus Diagnostics, Mumbai, India
3Namco Cancer Hospital, Nashik, India
4Government Medical College, Miraj, India
*Corresponding author: Nagesh Madnoorkar, Surgical Oncology, Vasundhara Cancer Clinic, Nashik, India
Received: 06 October 2023; Accepted: 17 November 2023; Published: 27 November 2023
© 2023 The Authors. This is an open-access article and is distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Abstract
Neuroendocrine tumors of the head and neck region are extremely infrequent. Small cell neuroendocrine carcinoma (NEC) of the tonsil is almost unheard of and carries a poor prognosis. There is no standard treatment protocol with regard to this tumor type. We present a 74-year-old male with complaints of odynophagia and swelling on the right side of the neck for one month. Physical examination showed a right neck level II lymph node with an ulceroproliferative mass involving the (R) tonsillar fossa, uvula, soft palate, and obstructing the oropharynx. MRI showed a right tonsillar mass measuring 3.4 × 3.3 × 1.4 cm with an ipsilateral level II lymph node measuring 2.7 × 1.9 cm. PET-CT scan showed a metabolically active right tonsillar lesion with a right level II lymph node. Histopathological examination revealed small cell NEC. On immunohistochemistry, tumor cells were strongly positive for PanCK, synaptophysin, chromogranin, CD56, and p16. Tumor cells were negative for CD45, CK7, CK20, and EBV-LMP. Ki-67 was 80%. The patient was treated with cisplatin and etoposide-based chemotherapy, and the tumor showed a very good response.
Keywords
neuroendocrine carcinoma, small cell carcinoma, tonsil, immunohistochemistry
Abbreviations
NECs: neuroendocrine carcinomas
1. Introduction
Neuroendocrine carcinomas (NECs) are rare tumor entities that arise from diffuse neuroendocrine cell systems. NECs occur mainly in the lungs, gastrointestinal tract, and genitourinary system [1]. Primary NECs of the head and neck are an uncommon and heterogeneous group of neoplasms and are categorized by WHO as a) well-differentiated (WD-NEC), b) moderately differentiated (MD-NEC), and c) poorly differentiated (PD-NEC) with small cell and large cell types [2]. A small cell type of NEC is a high-grade tumor that has aggressive behavior with a poor prognosis. In the head and neck, the larynx is a relatively common site for the occurrence of small cell carcinoma, followed by salivary glands, nasal cavity, and paranasal sinuses [3]. Small cell NECs of palatine tonsils are extremely rare, and limited cases have been reported so far. Due to its rarity, treatment strategy remains challenging. Here in this report, we describe a case of small cell NEC of the right tonsil, along with a review of the literature.
2. Case Report
A 74-year-old male without any co-morbidity presented in our outpatient department with a history of pain while swallowing from 3 months, which was gradual in onset, progressive, moderate to severe in intensity, and intermittent with no aggravating or relieving factors. The patient also had painless right neck swelling from 2 months. Local examination of the oropharynx revealed a 3 × 3 cm ulceroproliferative mass involving the R tonsillar fossa extending to the uvula, soft palate, and obstructing the oropharynx (Figure 1). Right lymph node level II was palpable, measuring 2.0 × 1.5 cm in size, non-tender, and firm to hard in consistency.
 Figure 1: Local examination of oropharynx showing tonsillar mass.
Figure 1: Local examination of oropharynx showing tonsillar mass.
MRI of the oral cavity revealed a 3.4 × 3.3 × 1.4 cm right tonsillar mass with moderate enhancement and right level II lymph node involvement measuring 2.7 × 1.9 cm (Figures 2 and 3). A multiple-punch biopsy of the right tonsillar mass was done. Histopathological sections showed sheets and loosely cohesive groups of monotonous cells with increased N:C ratio and scanty cytoplasm. The tumor cells were strongly positive for PanCK, synaptophysin, chromogranin, CD56, and p16 and were negative for CD45, CK7, CK20, and EBV-LMP on immunohistochemical staining (Figures 4 and 5). PET-CT was also done that showed metabolically active right tonsillar region with right level II neck node thus confirming the diagnosis of SC-NEC of right tonsil with TNM staging as T2N1M0 with stage II.
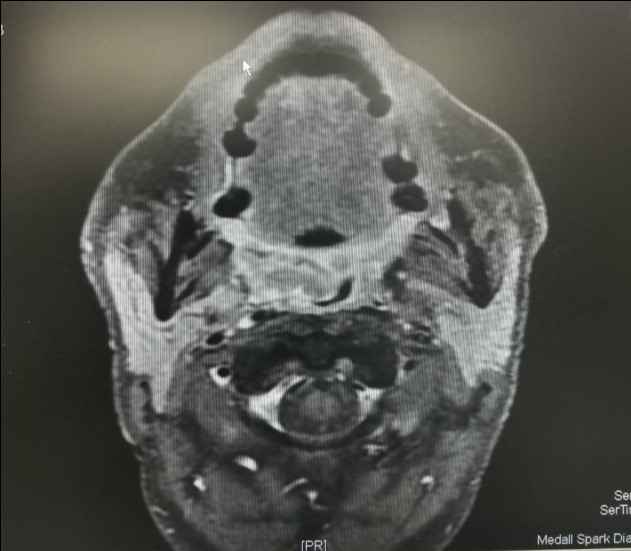 Figure 2: Axial scan sections showing right tonsillar mass.
Figure 2: Axial scan sections showing right tonsillar mass.
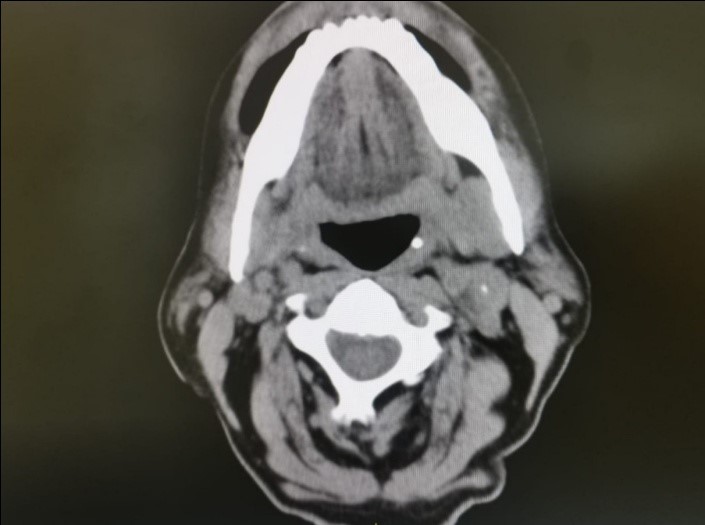 Figure 3: Coronal scan sections showing right tonsillar mass.
Figure 3: Coronal scan sections showing right tonsillar mass.
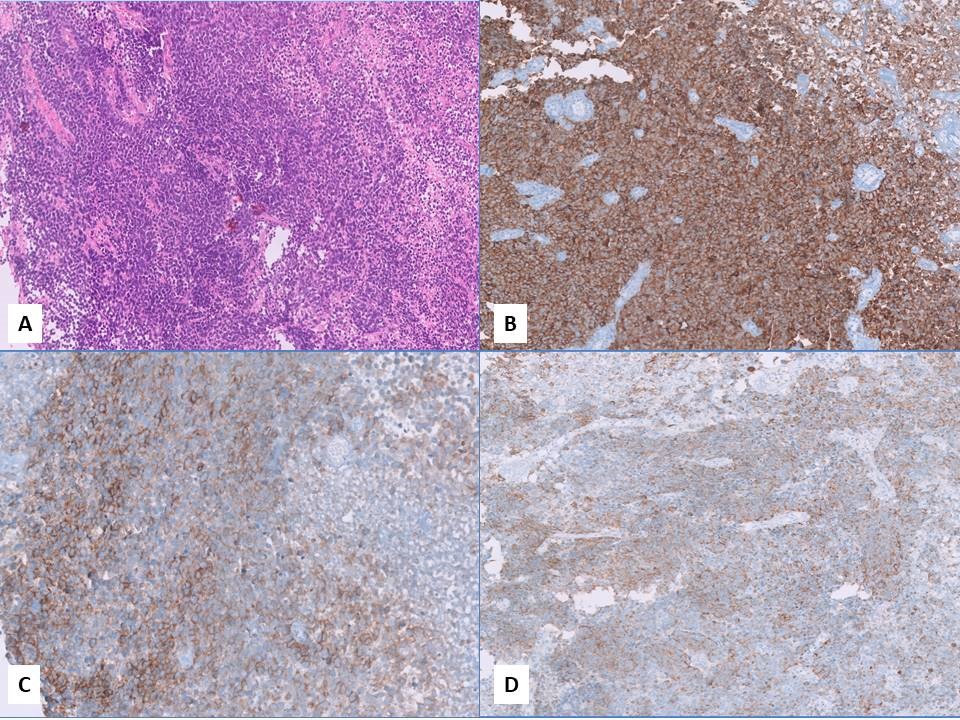 Figure 4: A) Sheets of atypical round cells with raised N:C ratio, high mitotic activity, H.E, 40X; B) Synaptophysin highlights the tumor cell; C) CD56 highlights the tumor cell; D) Pan cytokeratin highlights the tumor cell.
Figure 4: A) Sheets of atypical round cells with raised N:C ratio, high mitotic activity, H.E, 40X; B) Synaptophysin highlights the tumor cell; C) CD56 highlights the tumor cell; D) Pan cytokeratin highlights the tumor cell.
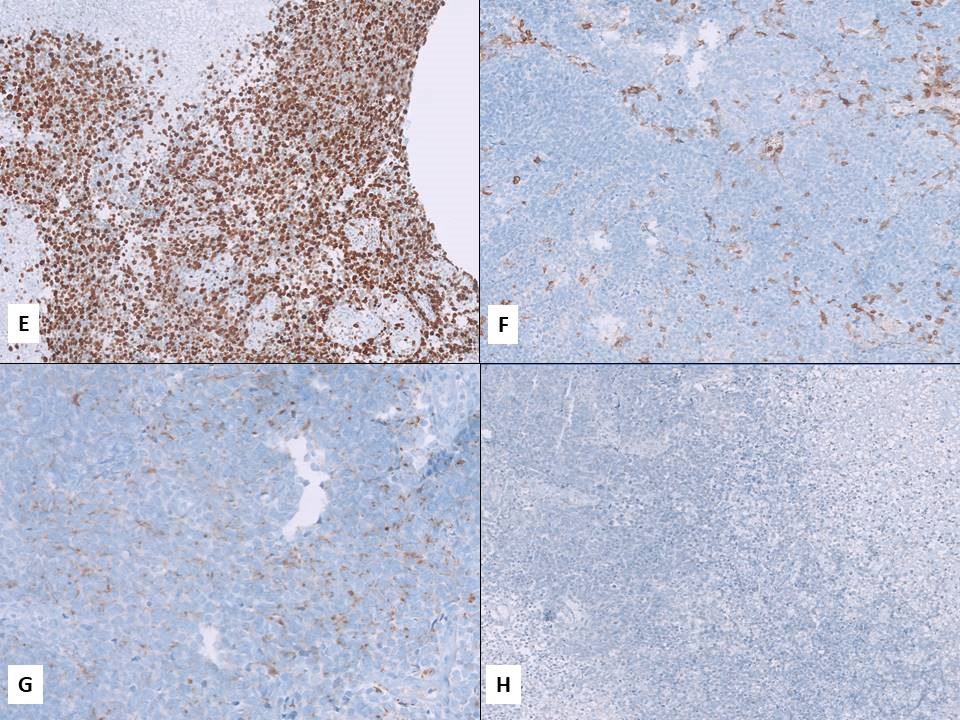 Figure 5: E) Ki-67 upto 80%; F) CD45 negative in tumor cell; G) Chromogranin highlights the tumor cell (weak staining); H) Cytokeratin 7 negative in tumor cell.
Figure 5: E) Ki-67 upto 80%; F) CD45 negative in tumor cell; G) Chromogranin highlights the tumor cell (weak staining); H) Cytokeratin 7 negative in tumor cell.
The patient received 2 cycles of induction chemotherapy with cisplatin and etoposide intravenously, followed by concurrent chemoradiation therapy. After treatment, the primary tumor had shrunken remarkably (Figure 6). Post-treatment CT scan was done which also showed a complete regression of the tumor (Figure 7). The patient is followed up every 3 months.
 Figure 6: Post-treatment examination of oropharynx showing regression of tonsillar tumor.
Figure 6: Post-treatment examination of oropharynx showing regression of tonsillar tumor.
Figure 7: Post-treatment axial scan showing complete regression of tumor.
3. Discussion
NECs are a spectrum of tumors, ranging from well-differentiated carcinoid tumors to poorly differentiated small cell carcinomas. Tumors are categorized as neuroendocrine when histology shows neuroendocrine differentiation, epithelial differentiation (either by virtue of arising in an epithelial – or mucosal-lined passage or positive immunohistochemical staining for cytokeratin), and immunohistochemical positivity for neuroendocrine markers (CD56/N-CAM, synaptophysin or chromogranin) [4].
Olofsson et al. reported the first case of primary extrapulmonary NEC arising in the head and neck [5]. Since then, it has been reported at multiple sites of the head and neck. Small cell NEC that primarily occurs in the tonsil is extremely rare. Three cases of small cell NEC in the tonsil were initially reported by Koss et al. [6]. It is mostly seen in the 5th and 7th decade of life and is twice as prevalent in males as females. Symptoms are associated with local invasion; however, paraneoplastic syndromes (commonly syndrome of inappropriate secretion of antidiuretic hormone) have also been reported. The tumor can also metastasize to the liver, lungs, bone, brain, and skin [7]. Diagnosis of small cell NEC depends on histopathological examination and immune histochemical staining. On microscopy, hallmarks of small cell NEC include small round to oval cells packed in sheets, cords, or ribbons with hyperchromatic nuclei, sparse cytoplasm, high nuclear/cytoplasmic ratio, and frequent necrosis and mitosis. On immunohistochemistry, positive staining of general neuroendocrine markers, including synaptophysin, chromogranin, NSE, and CD56, provide evidence of neuroendocrine differentiation of tumor cells [8].
Various treatment modalities for small cell NEC of the tonsil are surgical resection, radiotherapy, chemotherapy, or some combination of them. However, due to limited cases and sparse data, definite treatment management has not been well established. A previous study reported that extrapulmonary small cell carcinoma responded well to both chemotherapy and chemo-radiotherapy, similar to small cell carcinoma of the lung. However, a poor prognosis remains due to its strong metastatic potential. Thus, patients with small cell NEC should be treated with chemotherapy to prevent early metastasis. Platinum-based regimens like CDDP and etoposide are most commonly used in recent years. The new chemotherapeutic agent irinotecan has shown a significant effect against small cell lung cancer and has been reported in a case report of small cell NEC arising from the tonsil [9].
The present case was successfully treated with chemotherapy. The patient received six cycles of cisplatin combined with etoposide and showed a complete response as the tumor was fully resolved. However, due to the high chance of recurrence, the patient is followed up every 3 months.
4. Conclusion
Small cell NEC of the tonsil is extremely rare and highly aggressive, with a poor prognosis. Standard treatment protocol remains uncertain, while chemotherapy with etoposide and platinum followed by concurrent chemo-radiation seems to be the relatively appropriate option.
References
- Jang H, Yuk SM, Kim JO, et al. A rare case of primary malignant small cell carcinoma combined with urothelial cell carcinoma in the ureter. World J Surg Oncol. 2013;11(1):181.
- Perez-Ordonez B, Bishop JA, Gnepp DR, et al. Neuroendocrine Tumors. In: El-Naggar AK, Chan JKC, Grandis JR, et al. eds. WHO Classification of Head and Neck Tumors. 4th ed. Lyon: IARC; 2017. P. 95-98.
- Renner G. Small cell carcinoma of the head and neck: a review. Semin Oncol. 2007;34(1):3-14.
- Bellizzi AM. Immunohistochemistry in the diagnosis and classification of neuroendocrine neoplasms: what can brown do for you? Hum Pathol. 2020;96:8-33.
- Olofsson J, Van Nostrand AW. Anaplastic small cell carcinoma of larynx. Case report. Ann Otol Rhinol Laryngol. 1972;81(2):284-87.
- Koss LG, Spiro RH, Hajdu S. Small cell (oat cell) carcinoma of minor salivary gland origin. Cancer. 1972;30(3):737-41.
- Bates T, McQueen A, Iqbal MS, et al. Small cell neuroendocrine carcinoma of the oropharynx harbouring oncogenic HPV-infection. Head Neck Pathol. 2014;8(1):127-31.
- Sen R, Bhutani N, Saini R, et al. ‘Primary small cell carcinoma of tonsil: An extreme rarity.’. Ann Med Surg (Lond). 2019;44:29-32.
- Segawa Y, Nakashima T, Shiratsuchi H, et al. Small cell carcinoma of the tonsil treated with irinotecan and Cisplatin: a case report and literature review. Case Rep Oncol. 2011;4(3):587-91.
