Abstract
Purpose: To describe the case of a uniocular patient with advanced primary open-angle glaucoma (POAG) and age-related cataract in the right eye and microphthalmic left eye.
Methods: A 73-year-old one-eyed man presented with four years of painless, progressive dimness of vision in the right eye. The vision was 6/18 in the right eye, whereas the left eye had no light perception (NLP). In the left eye, severe ptosis and microphthalmos were detected, while the right eye had age-related cataracts, an open anterior chamber angle, intraocular pressure (IOP) of 30 mmHg, and progressive glaucomatous optic neuropathy.
The IOP was dropped to 22 mmHg after a topical timolol maleate (0.5%), brimonidine tartrate (0.2%), and brinzolamide (1%). As the patient had mature cataract, advanced glaucomatous optic nerve damage, target IOP was not reached, and adherence issues with antiglaucoma medications (AGM), the decision was made to proceed with cataract extraction combined with augmented trabeculectomy with mitomycin-C (MMC).
Results: There were no intraoperative complications. Over one year, the IOP was maintained in the 12–14 mmHg range without AGM.
Conclusion: In advanced glaucoma patients, combined phaco-trabeculectomy operations can considerably lower IOP and drug load or compliance concerns with antiglaucoma drugs. This case represented an efficient and safe surgical technique for uniocular advanced POAG, particularly in a developing country like Bangladesh.
Keywords
unilateral glaucoma, open-angle glaucoma, microphthalmos, phaco-trabeculectomy, Bangladesh
Abbreviations
POAG: primary open-angle glaucoma, NLP: no light perception, IOP: intraocular pressure, AGM: antiglaucoma medications, MMC: mitomycin-C, OCT: optical coherence tomography, RNFL: retinal nerve fiber layer
1. Introduction
Open-angle glaucoma is a degenerative optic neuropathy characterized by optic nerve head excavation and visual field abnormalities with an open anterior chamber angle [1]. Mechanical trauma to the optic nerve occurs in primary open-angle glaucoma (POAG) due to high intraocular pressure (IOP), which is recognized to be a major component in the development and progression of glaucoma [1]. The pathophysiology is unknown; however, it is likely to incorporate a wide variety of degenerative events that share the final common route of progressive loss of retinal ganglion cells with axons [2].
As glaucoma damage is permanent, the best possible care now depends on early diagnosis and treatment to reduce the risk of development and progression of vision impairment. Traditionally, the first-line therapy for glaucoma has been medical care with topical IOP-lowering medications. However, current guidelines, such as those issued by the United Kingdom’s National Institute for Health and Care Excellence (NICE), suggest that surgery may be an acceptable first-line therapy for individuals with advanced glaucoma at the time of diagnosis [3].
Microphthalmos occurs when the eye is smaller than normal by at least two standard deviations (SD) and can be complicated or simple depending on the presence or absence of other ocular anatomical abnormalities. The birth prevalence of microphthalmia has been reported to be 14 per 100,000 people. Anophthalmia can coexist with microphthalmia in one-third of cases [4].
The aetiology of microphthalmia is complicated, involving gestational infections, environmental, monogenic, and chromosomal disorders. Microphthalmia is substantially more common in newborn infants with low birth weights and gestational ages. SOX2 has been recognized as a significant cause among monogenic causes. PAX6, OTX2, CHX10, and RAX are additional linked genes [5].
A combination of clinical features, histopathological examination, imaging (ultrasonography and CT/MR scanning), and genetic analysis can be used to make a diagnosis both before and after birth.
McLean’s research for orbital cyst with microphthalmos documented the treatment protocol employed at Moorfields Eye Hospital, which is primarily focused on the early and intensive use of conformers and eventually replaced by an orbital implant and ocular prosthesis [6].
The purpose of this research is to describe the case of a microphthalmic one-eyed patient with advanced glaucoma and cataract who displayed well-controlled IOP while preserving good vision following phaco-trabeculectomy enhanced with mitomycin-C (MMC) without any medication load.
2. Case Presentation
A 73-year-old male presented with painless, gradual dimness of vision in the right eye for the last 4 years. He also gave a history of no vision in his left eye since birth and no history of trauma or surgery to his left eye, verified by his brother, who brought him for an eye check-up. There was no history of consanguineous marriage and the other sibling was normal, no other chronic medical or systemic illness was present. There were no clinical signs of systemic connections such as facial abnormalities, webbed hands, lid coloboma, preauricular skin tags, cleft lip, hydrocephalus, microcephaly, or convulsions.
On ocular examination, his left eye showed severe ptosis (Figure 1A), the best corrected visual acuity in the right eye was 6/36 (with -1.75 DSph), and no light perception (NLP) in the left eye. Central corneal thickness (CCT: 563 microns) corrected IOP was 30 mmHg in the right eye by Goldmann applanation tonometry.
On slit lamp examination, the right eye showed grade 3 nuclear sclerosis with cortical changes in the lens and a sectoral anterior capsular fibrosis (Figure 1B). The left eye showed microphthalmia (Figure 1C), but the ocular adnexa was in normal condition. Gonioscopy of the right eye showed a grade 4 open anterior chamber angle in all four quadrants with no notable pathological changes (Figure 1D).
Dilated fundus examination of the right eye showed advanced glaucomatous optic nerve changes with tigroid fundus (Figure 1E), supported by Humphrey visual field change (dense superior arcuate scotoma) (Figure 2A) and optical coherence tomography (OCT) of the optic nerve head showed extensive thinning of the retinal nerve fiber layer (RNFL) (Figure 2B).
B-scan ultrasonogram of the left eye showed dense vitreous opacities with thickened sclera which persisted in both high and low gain and a short axial length of 9.77 mm (Figure 2C and 2D).
The patient was prescribed a topical combination of timolol maleate (0.5%) and brimonidine tartrate (0.2%) twice daily and brinzolamide (1%) thrice daily in his right eye. After 15 days of initiating antiglaucoma medications (AGM), IOP dropped down to around 22 mmHg, and the patient underwent combined phaco-trabeculectomy augmented with 0.1 ml of 0.2mg/ml of MMC (Kyowa Hakko Kirin Co, Ltd., Tokyo, Japan) for 30 seconds.
The postoperative treatment regime was topical moxifloxacin (0.5%) 4 times daily for 1 month, prednisolone (1%) 2 hourly for 7 days, then 4 hourly for 7 days, 6 hourly for 7 days and 8 hourly for 7 days, and atropine sulphate (1%) 8 hourly for 7 days.
Postoperative day (POD) 1 showed visual acuity of 6/24 with clear cornea, pharmacologically (atropine sulphate 1%) dilated pupil, well-centered single-piece intraocular lens (IOL) in the bag, surgical peripheral iridectomy at 12 o’clock position and diffuse bleb formation (Figure 3A and 3B) with IOP of 12 mmHg without any AGM.
He was on regular follow-up for the last 1 year, maintaining good vision at distance (BCVA 6/18 with -0.75DCyl@90°) and near (N6 with +2.75 DSph) with IOP ranging from 12–14 mmHg without any topical antiglaucoma drops. The patient was also advised for left eye evisceration followed by a prosthetic eye implant, but he refused to do so.
 Figure 1: A) Severe ptosis of the left eye; B) Cataract in the right eye; C) Microphthalmic left eye; D) Grade 4 anterior chamber angle in gonioscopy of the right eye; E) Glaucomatous optic nerve damage with tigroid fundus.
Figure 1: A) Severe ptosis of the left eye; B) Cataract in the right eye; C) Microphthalmic left eye; D) Grade 4 anterior chamber angle in gonioscopy of the right eye; E) Glaucomatous optic nerve damage with tigroid fundus.
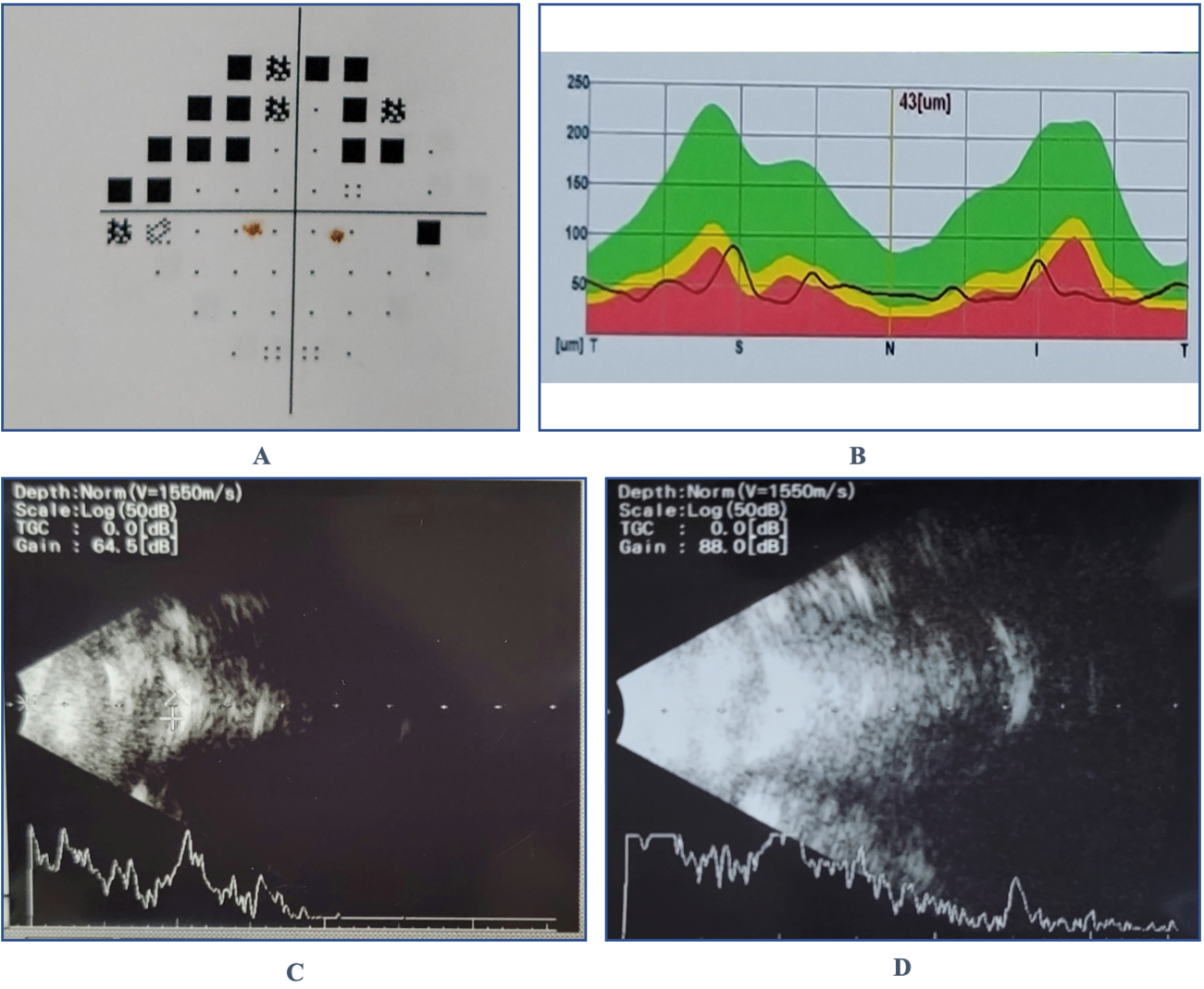 Figure 2: A) Dense superior arcuate scotoma in pattern deviation map of the Humphrey visual field of the right eye; B) Thinning and loss of double-hump pattern of the retinal nerve fiber layers in OCT of the right eye; C) and D) Dense vitreous opacity with thickened sclera in both high and low gain B-scan ultrasonogram of the left eye.
Figure 2: A) Dense superior arcuate scotoma in pattern deviation map of the Humphrey visual field of the right eye; B) Thinning and loss of double-hump pattern of the retinal nerve fiber layers in OCT of the right eye; C) and D) Dense vitreous opacity with thickened sclera in both high and low gain B-scan ultrasonogram of the left eye.

Figure 3: At 1st postoperative day following phaco-trabeculectomy surgery: A) Surgical PI at 12 O’clock position in a pseudophakic eye; B) Visible single-stitch at the apex of the triangular scleral flap under the diffuse bleb.
3. Discussion
At the time of presentation, the patient, in this case, had advanced glaucomatous damage, as evidenced by the significant loss of neural tissue on optic disc examination, the extreme thinning of the RNFL on OCT, and the functional deficit, with a visual acuity of 6/36. A low target pressure is needed to reduce the risk of visual loss in such a severe disease at the time of presentation, which indicates a poor prognosis. With no expectation of visual recovery, phaco-trabeculectomy with MMC surgery was offered with the sole objective of preventing vision loss.
We started topical antiglaucoma drugs to preserve vision in the right eye, where the pressure remained high at 22 mmHg after maximal tolerated glaucoma treatment. Although cataract surgery usually lowers IOP, it is inadequate in situations of uncontrolled glaucoma. Furthermore, glaucoma patients undergoing cataract surgery have a higher prevalence of postoperative IOP spikes with IOPs over 30 mmHg, which poses a substantial danger in eyes with pre-existing glaucoma [7].
With or without AGM, combined phaco-trabeculectomy provides superior 24-hour IOP control and protects against postoperative IOP spikes [8]. According to the Otago Glaucoma Surgery Outcome Study, trabeculectomy and simultaneous cataract extraction resulted in improved vision [3]. For these reasons, we decided to perform phaco-trabeculectomy.
In our case, IOP dropped from 30 mmHg preoperatively to 12 mmHg following phaco-trabeculectomy and maintained in the 12–14 mmHg range for a year without glaucoma drops. This decline in IOP and visual recovery may look spectacular, but it must be noted that the visual prognosis remains poor due to extensive glaucomatous damage in the right eye.
Microphthalmos is one of the most prevalent ocular organogenetic abnormalities, resulting in a failure of overall eye development; several forms have been clinically described. Other ocular abnormalities may complicate it [9]. But this patient did not have any developmental abnormalities other than left microphthalmos.
Elder [10] discovered that microphthalmic eyes with a corneal diameter of 5 mm or less at birth were related to no perception of light in 81% of cases. Our patient had no vision in the left microphthalmic eye.
Simple microphthalmia manifests as a typical small globe with a short axial length and normal signal/density properties of the lens and vitreous in a smaller orbit than usual [4]. This patient had a shorter axial length of 9.77 mm with vitreous opacities in the B-scan ultrasonogram.
Instead of improving sight, therapy aims to improve cosmetic appearance and maximize existing vision, if any. This patient resisted our recommendation to undergo evisceration followed by an orbital implant, and an ocular prosthesis.
4. Conclusion
To the best of our knowledge, this is the first case of phaco-trabeculectomy enhanced with MMC in a patient with monocular advanced POAG and age-related cataract in the right eye with left microphthalmos. This phaco-trabeculectomy reduced IOP and medication usage while improving vision without any intraoperative issues. This instance further supports the notion that early surgery be considered in individuals with advanced glaucoma, particularly in developing countries like Bangladesh. The patient’s aesthetic appearance would be considerably improved with an orbital implant and ocular prosthesis.
Acknowledgment
Vitreo-retina Department of Ispahani Islamia Eye Institute and Hospital, Dhaka, Bangladesh.
Author Contributions
SJK- treating ophthalmologist, took part in drafting, gave final approval of the version to be published; MII- clinical evaluation, treating surgeon, concept and design, literature review, writing of the article, critical review of the manuscript, journal submission; SM- treating ophthalmologist, took part in drafting; AR- treating ophthalmologist, took part in drafting.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Approval and Consent to Participate
Institutional approval was not required for the publication of this case.
Consent for Publication
Informed written consent was obtained from the patient for the publication of this case report and accompanying images.
Financial Support
Conflicts of Interest
References
- Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008;19(2):85-8.
- Myron Yanoff M, Sassani JW. Glaucoma. In Ocular Pathology. 2015; pp. 555–588.e7. Elsevier.
- Foulsham WS, Fu L, Tatham AJ. Visual improvement following glaucoma surgery: a case report. BMC Ophthalmology. 2014;14(1):162.
- Verma AS, FitzPatrick DR. Anophthalmia and microphthalmia. Orphanet J Rare Dis. 2007;2(1):47.
- Faivre L, Williamson KA, Faber V, et al. Recurrence of SOX2 anophthalmia syndrome with gonosomal mosaicism in a phenotypically normal mother. Am J Med Genet A. 2006;140(6):636-9.
- McLean CJ, Ragge NK, Jones RB, et al. The management of orbital cysts associated with congenital microphthalmos and anophthalmos. Br J Ophthalmol. 2003);87(7):860-863.
- Iancu R, Corbu C. Intraocular pressure after phacoemulsification in patients with uncontrolled primary open angle glaucoma. J Med Life. 2014;7(1):11-16.
- Liaska A, Papaconstantinou D, Georgalas I, et al. Phaco-trabeculectomy in controlled, advanced, open-angle glaucoma and cataract: parallel, randomized clinical study of efficacy and safety. Semin Ophthalmol. 2014;29(4):226-35.
- Ghose S, Singh NP, Kaur D, et al. Microphthalmos and anterior segment dysgenesis in a family. Ophthalmic Paediatr Genet. 1991;12(4):177-82.
- Elder MJ. Aetiology of severe visual impairment and blindness in microphthalmos. Br J Ophthalmol. 1994;78(5):332-4.
