Farajirad M*1, Farajirad E2, Motlagh Pirooz F3 and Mohazzab Torabi S1
1Department of Neurosurgery, Mashhad University of Medical Sciences, Mashhad, Iran
2Resident Physician in Adult Neurology, University of Toronto, Canada
3Department of Neurosurgery, Islamic Azad University, Mashhad, Iran
*Correspondence: Mohammad Faraji-Rad, Department of Neurosurgery, Mashhad University of Medical Sciences, Mashhad, Iran
Received on 12 August 2023; Accepted on 09 October 2023; Published on 13 October 2023
Copyright © 2023 Farajirad M, et al. This is an open-access article and is distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Colloid cysts (CC) are infrequent and benign cystic formations located in the third ventricle proximate to the foramen of Monro. Although surgical resection is widely acknowledged as the standard approach for managing symptomatic large-sized CC, the necessity of surgical intervention for asymptomatic or minimally symptomatic cases remains a subject of ongoing debate.
Case Presentation: In this report, we present the case of a 34-year-old female patient who complained of severe headaches. She was totally alert with normal cranial nerves examination and acute papilledema. Magnetic resonance imaging (MRI) revealed a characteristic 12 mm-sized CC situated in the third ventricle. Furthermore, fluid-attenuated inversion recovery (FLAIR) MRI demonstrated severe hydrocephalus with periventricular edema. Surprisingly, the patient was thoroughly informed of the potential treatment options during the first visit, including the possibility of neurosurgical tumor resection. However, the patient expressed reluctance and declined to provide consent for the neurosurgical intervention at that time. Remarkably, subsequent MRIs conducted 18 months after the initial evaluation demonstrated a spontaneous reduction in cyst size from 12 mm to 2 mm.
Conclusion: The phenomenon of spontaneous regression in CC is an exceedingly rare event. For carefully selected, asymptomatic cases, an alternative management approach involving regular imaging surveillance and frequent neurological assessments could be considered. However, the decision-making process should be meticulous, with a comprehensive evaluation of the associated risks and potential benefits of surgical intervention vs. conservative observation tailored to each case. Further research and larger studies are warranted to validate the feasibility and long-term outcomes of this alternative management strategy.
Keywords
colloid cysts, hydrocephalus, regression
Abbreviations
CC: colloid cysts; MRI: magnetic resonance imaging; FLAIR: fluid-attenuated inversion recovery
Introduction
Colloid cysts (CC) are rare, benign cystic growths located in the third ventricle near the foramen of Monro. They represent about 2% of all brain tumors and are characterized by an epithelium-lined fibrous capsule containing proteinaceous material [1]. Radiologically, they appear as well-circumscribed lesions with variable density on CT and intensity on both T1 and T2 weighted magnetic resonance imaging (MRI) [2].
CC can manifest in various ways, with some remaining asymptomatic for long periods, while others may cause symptoms like headaches, gait disturbances, nausea, blurred vision, and urinary incontinence. They can also be associated with acute or chronic hydrocephalus, and, in certain cases, they might suddenly obstruct the foramen of Monro, leading to serious consequences such as drop attacks or sudden death [3].
Although the exact cause of CC is still debated, they are generally believed to be congenital in nature. While they can be found in individuals of various ages, they are more commonly observed in adults, particularly those between their 30s and 50s [4]. CC may have a familial predisposition, although their incidence decreases with age after adulthood [5].
Neurosurgical management of symptomatic CC typically involves surgical resection, even in the absence of hydrocephalus. For patients with minimal or no symptoms, a cautious approach is necessary, and the cyst may either be surgically removed or closely monitored through serial neuroimaging. Spontaneous regression of CC is exceedingly rare [6].
This case report presents a compelling instance of a CC that underwent spontaneous regression, shedding light on this infrequent phenomenon and exploring the associated pathological mechanisms through a review of relevant literature. Understanding such nuances in CC management can lead to better patient outcomes and enhance our knowledge and practice in the field of neurosurgery.
Case Report
We present one distinct case report involving a patient diagnosed with CC, illustrating their diverse clinical trajectories and management outcomes.
Our case involves a 34-year-old female patient with no underlying medical conditions who incidentally presented with severe headaches and nausea in February 2021. On examination, she was alert (GCS:15/15) with normal cranial nerves examination but acute papilledema. The brain MRI unveiled a 12 mm-sized CC positioned in the third ventricle. The cyst appeared as a well-defined, round lesion in the right foramen of Monro and the upper third ventricle. On T1-weighted images, the cyst showed isointensity, whereas, on T2-weighted images, it predominantly exhibited hyperintensity with a hypointense focus within the lesion. The signal intensity pattern on fluid-attenuated inversion recovery (FLAIR) images was consistent, likely attributed to the highly proteinaceous nature of the cyst fluid and acute hydrocephalus and periventricular edema (Figure 1).
The patient was thoroughly informed of the potential treatment options during the first visit, including the possibility of neurosurgical tumor resection. However, the patient expressed reluctance and declined to provide consent for the neurosurgical intervention at that time.
Given the patient’s preference for conservative management, close monitoring with regular imaging follow-ups was decided upon by the medical team. Over the course of 18 months after the initial assessment, subsequent MRI follow-ups demonstrated a spontaneous regression of the CC, with its size reducing from 12 mm to 2 mm. Despite the reduction in size, the patient continued to remain asymptomatic and showed no signs of neurological deficits.
Continuing with the conservative approach, further follow-up imaging at 30 months showed a stable cyst size with no significant changes. Throughout this period, the patient did not develop any clinical symptoms related to the CC, and the absence of neurological deficits persisted (Figure 2).
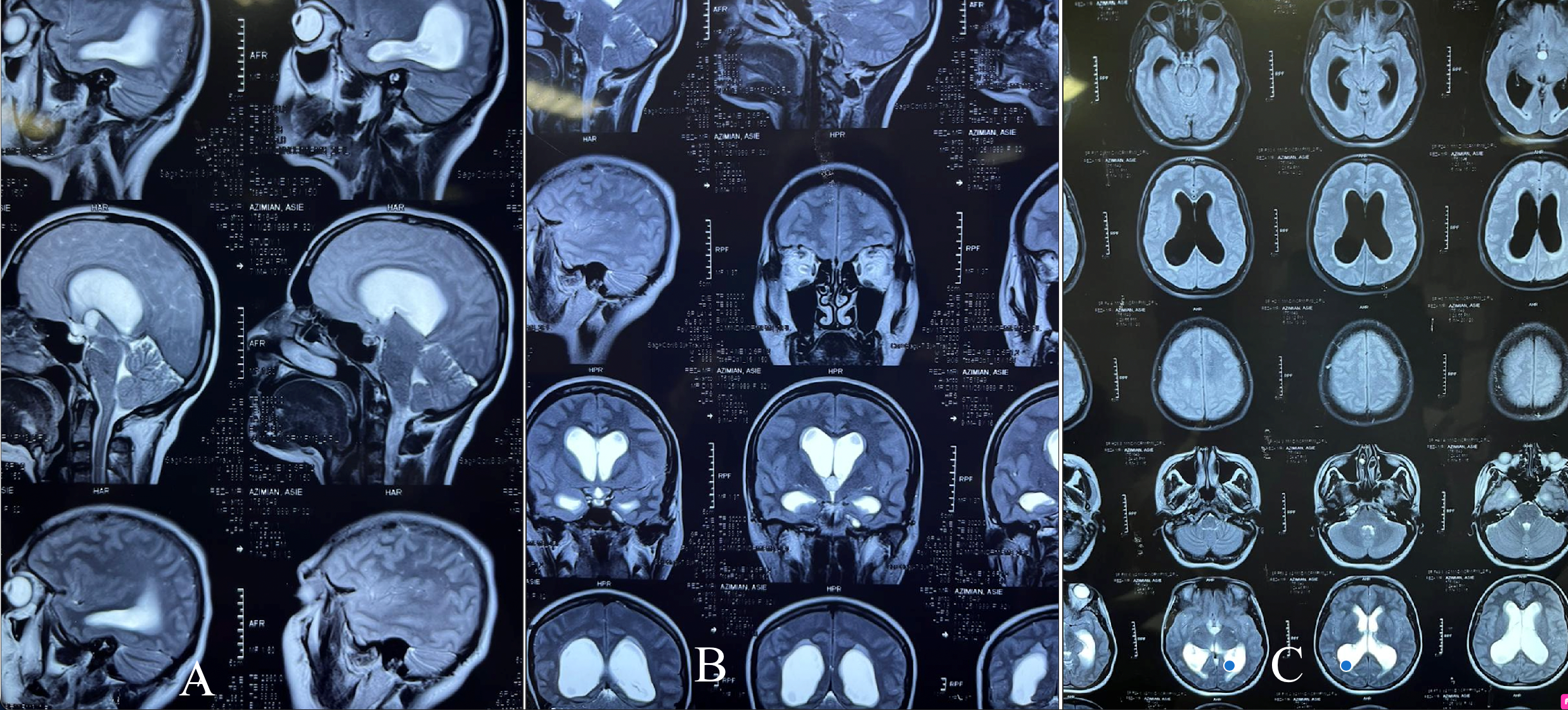 Figure 1: Primary MRI in T2 sagittal (A), coronal (B), and FLAIR axial (C).
Figure 1: Primary MRI in T2 sagittal (A), coronal (B), and FLAIR axial (C).
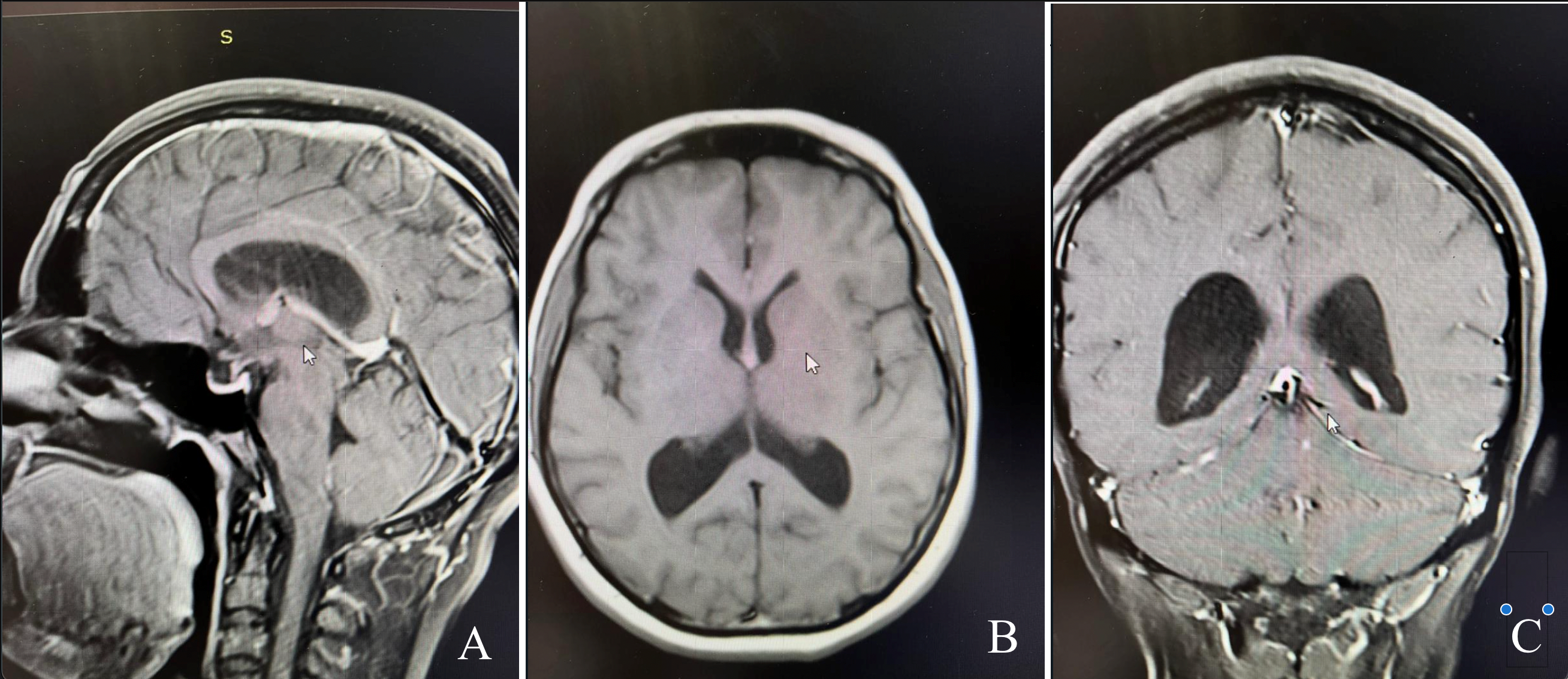 Figure 2: Secondary (after 18 months) MRI in T2 sagittal (A), coronal (B), and axial (C).
Figure 2: Secondary (after 18 months) MRI in T2 sagittal (A), coronal (B), and axial (C).
Discussion
The pathophysiological mechanisms underlying the progression of CC remain a topic of controversy and limited understanding. Although the majority of incidentally discovered cases tend to remain stable and asymptomatic [5], there is a potential risk of cyst enlargement leading to acute obstructive hydrocephalus and even death, particularly if the foramen of Monro becomes occluded. The estimated rate of rapid clinical deterioration varies widely, ranging from 3–35%, with a 5–38% risk of mortality [6]. However, it is worth noting that most cases in these series initially presented with symptoms [7].
Multiple theories have been proposed to explain rapid cyst enlargement. Intra-cystic hemorrhage is an infrequent cause of progression observed following exercise or head trauma [8]. Additionally, fatalities associated with air travel have raised the possibility of cabin pressure alterations triggering cyst expansion [9]. Furthermore, patients with CC, even if their cyst size remains unchanged on imaging, may still be at risk of developing acute hydrocephalus. The ball-valve mechanism, supported by cases of post-traumatic acute hydrocephalus, suggests that the cyst may obstruct the foramen of Monro, possibly due to shearing forces displacing the cyst towards the foramen or aqueduct of Sylvius [10]. Thus, stability in cyst size on imaging does not eliminate the risk of acute hydrocephalus development [11].
Presently, the standard management approach for small incidental CC involves radiological surveillance. However, the optimal frequency of imaging remains unclear, considering that a minority of cases may exhibit a catastrophic course. One asymptomatic patient who developed ventriculomegaly at 101 months chose to decline surgical treatment but later developed acute hydrocephalus after five months, leading to significant complications and eventual passing after four years. This highlights the risk of acute hydrocephalus even in cases with stable imaging findings [12].
To improve prognostication and identify high-risk patients, several scoring systems have been proposed. Beaumont et al. developed a 5-point Colloid Cyst Risk Score (CCRS) based on common risk factors identified in a retrospective analysis [13]. Further expanded this with an 8-point modified Colloid Cyst Risk Score (mCCRS), incorporating gender, fronto-occipital horn ratio, and further sub-categorizing cyst size [7]. Nevertheless, these scoring systems are relatively new and require further validation before being widely incorporated into clinical practice [14].
The long-term natural history of asymptomatic CC remains uncertain. Cases have been reported where progression occurred even after several years [15]. Therefore, continuous radiological and clinical surveillance is recommended for the long term. An annual review may be a prudent approach, although the low case numbers currently limit a definitive recommendation.
Patient education is a critical aspect of management, regardless of cyst size and stability, as radiological surveillance can be asymptomatic. Educating patients on warning symptoms and when to seek medical attention is crucial. Early recognition of symptoms played a pivotal role in our first case, where prompt surgical intervention resulted in a favorable outcome [16].
The underlying pathophysiological cause of spontaneous regression is not well understood, but it has been postulated that cyst rupture may lead to cyst contents being absorbed into the ventricle, leaving only traces of the cyst wall. However, further research is required to fully comprehend the mechanisms behind spontaneous regression.
For asymptomatic CC, a careful definition of asymptomatic criteria is essential, as observation with regular follow-up imaging can be a viable treatment option. It is crucial to consider the patient’s perspective regarding symptoms, as perceptions of symptom severity may vary. Additionally, if the cyst size increases, signs of increased intracranial pressure should not be overlooked, and the patient should be educated accordingly.
Conclusion
In conclusion, managing CC poses significant challenges due to its complex pathophysiology. Radiological and clinical surveillance is crucial for all cases, even those with stable cyst size. Scoring systems can assist in identifying patients at higher risk for cyst progression, although further validation is required. Surgical resection remains the primary treatment for symptomatic or large CC, but observation with regular imaging may be appropriate for selected asymptomatic cases, some of which may undergo spontaneous regression. Patient education plays a pivotal role in recognizing warning symptoms and seeking prompt medical attention. Future research is necessary to improve our understanding of the natural history and mechanisms of spontaneous regression in CC.
References
- Hernesniemi J, Leivo S. Management outcome in third ventricular colloid cysts in a defined population: a series of 40 patients treated mainly by transcallosal microsurgery. Surg Neurol. 1996;45(1):2-14.
- Desai KI, Nadkarni TD, Muzumdar DP, et al. Surgical management of colloid cyst of the third ventricle–a study of 105 cases. Surg Neurol. 2002;57(5):295-302.
- Farooq MU, Bhatt A, Chang HT. Hemorrhagic colloid cyst in a 9-year-old girl. Pediatr Neurol. 2008;38(6):443-44.
- Bavil MS, Vahedi P. Familial colloid cyst of the third ventricle in non-twin sisters: case report, review of the literature, controversies, and screening strategies. Clin Neurol Neurosurg. 2007;109(7):597-601.
- Joshi SM, Gnanalingham KK, Mohaghegh P, et al. A case of familial third ventricular colloid cyst. Emerg Med J. 2005;22(12):909-10.
- Pollock BE, Schreiner SA, Huston J 3rd. A theory on the natural history of colloid cysts of the third ventricle. Neurosurgery. 2000;46(5):1077-081.
- Motoyama Y, Hashimoto H, Ishida Y, et al. Spontaneous rupture of a presumed colloid cyst of the third ventricle–case report. Neurol Med Chir (Tokyo). 2002;42(5):228-31.
- Osborn AG, Hedlund GL, Salzman KL. Osborn’s Brain. 2nd ed: Elsevier; 2017. Chapter 28: Nonneoplastic Cysts.
- Gbejuade H, Plaha P, Porter D. Spontaneous regression of a third ventricle colloid cyst. Br J Neurosurg. 2011;25(5):655-57.
- Peeters SM, Daou B, Jabbour P, et al. Spontaneous Regression of a Third Ventricle Colloid Cyst. World Neurosurg. 2016;90:704.e19-704.e22.
- Turel MK, Kucharczyk W, Gentili F. Spontaneous resolution of colloid cyst of the third ventricle: Implications for management. Asian J Neurosurg. 2017;12(2):203-206.
- Annamalai G, Lindsay KW, Bhattacharya JJ. Spontaneous resolution of a colloid cyst of the third ventricle. Br J Radiol. 2008;81(961):e20-2.
- Peeters SM, Daou B, Jabbour P, et al. Spontaneous Regression of a Third Ventricle Colloid Cyst. World Neurosurg. 2016;90:704.e19-704.e22.
- Magalhães-Ribeiro C, Mascarenhas L, Santos RB, et al. Spontaneous asymptomatic resolution of a third ventricle colloid cyst. Neurochirurgie. 2020;66(2):137-38.
- Zeineddine HA, Westmark K, Khanpara S, et al. Risk Analysis and Management of Third Ventricular Colloid Cysts. World Neurosurg. 2021;146:e1071-e1078.
- Cosgrove ME, Saadon J, Chesler DA. Colloid cyst curtailed: A case report of spontaneous colloid cyst regression. Surg Neurol Int. 2020;11:465.
