Abstract
Objective: Obesity is a very common health problem and is considered a global non-communicable disease by the World Health Organization (WHO). Modern-day obesity is mainly due to physical inactivity, a high-calorie diet, and a sedentary lifestyle. It is associated with a multitude of commodities, such as diabetes type II, cardiovascular disease, hypertension, and even cancer. Due to this, obese patients are more likely to present for health assessment and are more likely to require imaging. The size of these patients brings diagnostic challenges involving gantry size, image quality, and radiation exposure. This review article compiles all the challenges and new techniques to overcome them during the imaging of the obese.
Key findings: There are many challenges to imaging the obese, as mentioned. Each modality also has its own specific set of challenges. There have been efforts to overcome these shortcomings, and many manufacturers now produce machines with higher weight load capacity and many other features to improve imaging of the obese, as mentioned in this article.
Conclusion: Obese patients face unique challenges in medical imaging and intervention. Over the last few years, medical manufacturers, radiographers, and radiologists have recognized these issues and come up with innovative techniques to overcome these challenges.
Implications for practice: Technical challenges of imaging obese patients need to be known and addressed, as mentioned in this paper.
Keywords
obesity, imaging, radiologists, challenges, obese patients
Abbreviations
BMI: body mass index, CT: computerized tomography, MRI: magnetic resonance imaging, FDG: F-18 fluorodeoxyglucose, NM: nuclear medicine, PET: positron emission tomography
1. Introduction
As per the World Health Organization, the prevalence of overweight and obesity has doubled in the last three decades [1]. Obesity is defined as a body mass index (BMI) greater than 30 kg/m2. Being overweight is defined as having a BMI between 25 to 29.9 kg/m2. The high prevalence of obesity is due to physical inactivity, overeating, genetics, and socioeconomic factors [2]. It is associated with a higher prevalence of diabetes mellitus, diabetic nephropathy, cardiovascular diseases, and cancer. Due to this, patients with obesity are more likely to come to the hospital and more likely to undergo medical imaging [3]. Size is a challenge for the quality imaging of these patients. The current literature on imaging obese patients is low. The purpose of this article is to review the challenges in imaging the obese and the advances made to overcome these in the past few years.
2. Radiography
Imaging is affected by a patient’s weight, girth, and adipose tissue distribution [4]. Each imaging equipment has a maximum table weight and aperture limit. Medical software does not allow equipment to proceed with imaging if the permissible weight is crossed. Most manufacturers have now increased the permissible weight above 250 pounds for all types of radiological equipment, and some can accommodate up to a 500-pound patient. Seo et al. [5] state that patients with obesity get more radiation per study compared to a person with a normal BMI. This is because body thickness affects X-ray attenuation (Figure 1).
Many strategies mentioned in the literature to increase image exposure are derived from film-screen radiography, which is outdated. New digital and computed radiography techniques have wider exposure latitude than film-screen technology, and thus new models to improve image quality are required. Dose creep is a phenomenon of gradual acceptance of radiographers to use increasing radiation to improve image quality if radiographers are not trained in imaging this group of patients. Also, difficult patient positioning and locating bony landmarks to center the X-ray beam accurately also affect the image quality. Difficulty also occurs in achieving coverage of the anatomical area of interest due to their large size. For this, training needs to be provided on phantoms with increasing size to mimic patients with obesity. The patient needs to be positioned in a way so that the thinnest body fat layer is closest to the image receptor. Image receptor size is also a limiting factor, as even large 14 × 17-inch image receptor sizes are smaller for an obese patient. A solution to this is using multiple cassettes together to achieve coverage. Some of the techniques to improve image quality is using a Bucky grid, double exposure, increasing tube voltage, increasing film development speed, and adjusting window and level settings. Automatic exposure control (AEC) is an automated way to control the dose received on the image receptor. Exposure is automatically turned off once the optimum image quality is achieved. Compassionate care also needs to be provided to these patients by the radiographer despite facing stress in getting a good quality image [6]. Think aloud strategy is another decision-making technique in which the radiographers verbalize their thoughts while performing a radiograph on obese patients. This not only helps them to understand what they are doing but also others in the team to understand the exact steps in the procedure being performed and to prevent any mishaps during the procedure [5].
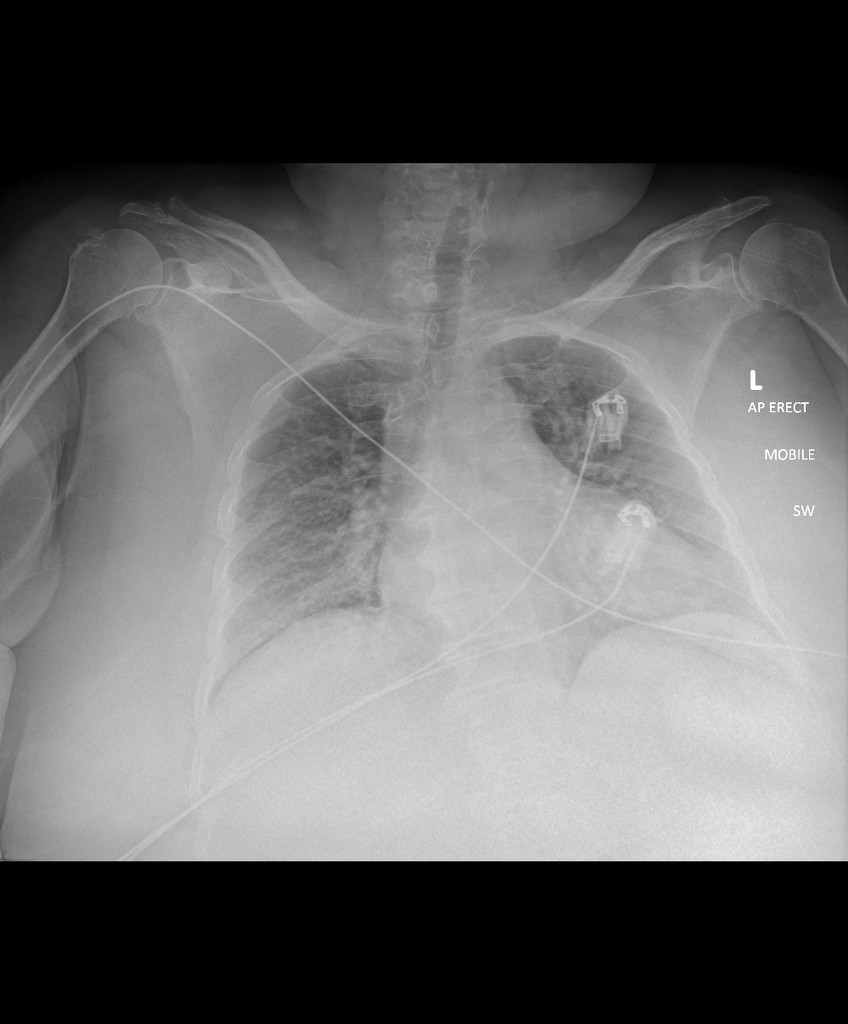 Figure 1: Radiograph of an obese patient shows haziness in both lungs due to soft tissue shadow. This can be misinterpreted as pulmonary edema or pneumonia.
Figure 1: Radiograph of an obese patient shows haziness in both lungs due to soft tissue shadow. This can be misinterpreted as pulmonary edema or pneumonia.
3. Fluoroscopy
Aperture diameter in fluoroscopy is important, as with computerized tomography (CT). Many times, hospitals are asked to image large post-op gastric bypass patients, and the aperture diameter of the fluoroscopy machine is the most important limiting factor. Apart from the weight limit, the additional problem with fluoroscopy tables is the table rotation. Adequate rotation might not be possible if the motor is not able to move the obese patient. Due to this, if fluoroscopy is not possible, then the study needs to be performed with only overhead radiographs, or the patient needs to be transferred to CT, as the allowed weight limit is larger and table rotation is not required.
4. Mammography
Attenuation due to obesity can lead to increased noise, decreased image contrast, and motion unsharpness. Larger breasts are also harder to compress during mammography [7].
5. Sonography
Obesity degrades image quality in three known ways (Figure 2). The first is due to the increased distance of organs from the skin surface, thus leading to the use of lower frequency probes with a restricted resolution. Secondly, there is increased attenuation of ultrasound waves while passing through fat. Ultrasound waves can get attenuated by up to 50% while traveling through 1 cm of fat [8]. Thirdly, the speed of ultrasound in fat compared to other human tissues is less. Using the lowest frequency transducers (15-2 MHz) to maximize penetration of depth, pushing in with the transducers to decrease the depth of adipose tissue, and placing transducers at the closest distance to the organ of interest are some of the techniques to improve ultrasound image quality.
Ultrasound transducers generally use a constant sound speed of 1.54 mm/micros. However, the body’s inhomogeneity and obesity lead to defocusing and clutter. Napolitano et al. [9] describe a sound speed correction technique to provide an automated way to adjust sound speed by using various trial sound speeds and then analyzing them to find the best image and then adjusting the sound speed of transducers accordingly for each body part. The advent of low-frequency curvilinear frequency probes (1-5 MHz) can allow better depth visualization (up to 30 cm). New crystal designs that maximize the efficiency of the piezoelectric crystal are available. Tissue aberration correction technology allows the system to detect altered beam penetration through fat tissue and to correct the image created to achieve better contrast and fewer artifacts. The application of tissue harmonics and pulse-inversion harmonics has been shown to produce a better image in obese patients [10,11].
 Figure 2: Ultrasound being performed in an obese patient.
Figure 2: Ultrasound being performed in an obese patient.
6. Computerized Tomography
Most CT machines also have a standard aperture which is not adequate for the girth of an obese patient. Extra-large gantry needs to be made separately for obese patients (Figure 3). An innovation that many hospitals use to measure a patient before putting on a gantry is to make them pass through a hula hoop to check their diameter. The diameter of the hula hoop is kept the same as the gantry diameter. Typical gantry diameters are 70 cm. However, larger bariatric gantry diameters are up to 85 cm. Table length also is important as it helps increase coverage in the z-direction. IV access for contrast injection may be difficult in obese patients. Some of the techniques include multiple tourniquets, using anatomic landmarks, and using warm compresses [12]. kVp, mAs, radiation dose, and noise index also have to be adjusted depending on patient size.
 Figure 3: Wide bore CT scanner for obese patients.
Figure 3: Wide bore CT scanner for obese patients.
7. Magnetic Resonance Imaging
These scanners have extra challenges as phased array coils also need to be accommodated inside the bore. The largest magnetic resonance imaging (MRI) machines have bore diameters of 70 cm. Some obese patients don’t fit these machines also. They are then referred to open MRI, which produces low-quality images (Figure 4).
Although the rate of attenuation for MRI is not as much as for X-ray beams or ultrasound waves, however, the signal-to-noise ratio may be affected. So, MR machines with higher field strength need to be used. A limited field of view is an additional challenge in the MRI of obese patients. This can cause wraparound artifacts. Solutions to address this problem are choosing the “no-wrap” option and adjusting the configuration of the field of view from rectangular to square configuration [13]. New MRI machines use matrix coils and a moving table, allowing for the creation of virtual eFOV, which is beneficial for MR angiography. There is a risk for obese patients of skin burns when their girth is so high that their skin is very close to the gantry [14]. In an obese ICU patient, who has sweat on their skin surface, the sweat can act as a conductor and increase the risk of burns. A cloth or cotton wool should be placed between their arms and the bore. Using saturation bands can reduce the noise created by excess subcutaneous fat [15].
 Figure 4: Open magnet MRI can accommodate obese patients.
Figure 4: Open magnet MRI can accommodate obese patients.
8. Nuclear Medicine/Positron Emission Tomography
Obese patients face technical challenges regarding the amount of weight-based nuclear medicine agents that can be administered. These are nowadays corrected by providing the maximum allowable dose to obese patients and by increasing gamma camera imaging times to maximize photon count. A common (PET) imaging agent is F-18 fluorodeoxyglucose (FDG). However, for PET imaging, an upper limit of the acceptable blood glucose level of 200 mg/dL is important for a diagnostic examination, as higher glucose blood levels, if rapidly corrected with insulin, can result in false-negative interpretations owing to increased muscle uptake of the tracer. Another challenge for the use of PET/CT, similar to contrast-enhanced CT or MR, is the requirement of a pre-scan fasting state. Doses of FDG often need to be increased in obese patients with diabetes to obtain adequate images, however, the Commission on Radiological Protection sets limits on administered doses. Dose limits can be overcome by increasing data acquisition; however, this leads to long scan times for patients and greater susceptibility to motion artifacts.
9. Interventional Radiology
There are many challenges in performing interventional radiology procedures on obese patients. These include difficulty visualizing targeted areas, inadequate instrument length, the inability of the patient to fit into CT and MRI scanners, increasing weight-based radiation dose, sedation of obese patients which is an anesthetic challenge, post-procedure recovery, and healing which is delayed in obese patients. Ultrasound-guided biopsies can lead to non-diagnostic samples in obese patients if the target area is not well visualized and the biopsy needle is not long enough to reach the target site through the layers of adipose tissue. The longest needle measures 25 cm and special instruments with longer lengths need to be manufactured for obese patients. Straps that hold the pannus out of the way while performing biopsies are needed. Increased interventional dose of more than 5 Gray in obese patients due to difficult procedures leads to a risk for skin burn. Some of the solutions for this include minimizing magnification and changing the frames per second from the default of 7.5 to 4 frames per second. Also rotating the beam, using pulsed fluoroscopy, and keeping the image intensifier close to the patient are some of the techniques to reduce radiation burns. Sedation for performing these procedures is also a challenge. Undersedation and oversedation are both potential hazards in obese patients due to the wrong dosage. Also, obstructive sleep apnea and difficult airway are potential challenges to airway access. It is important that the nursing staff and radiologists know about the risk of respiratory compromise in obese patients and that continuous monitoring with appropriate blood pressure cuffs is done. Lying the obese patient in a prone position can induce hypoxia, and positioning the patient in a lateral decubitus position for procedures such as percutaneous nephrostomy is more appropriate [16, 17]. Post-procedure obese patients have a greater risk for poor wound healing due to increased stress in the approximation of tissues as well as poor wound healing due to associated type II diabetes mellitus. Obese patients are less mobile and take longer to ambulate. They thus take a longer time to recover their pulmonary and peripheral circulatory function.
10. Special Challenges in Cancer Imaging
Cancer imaging poses special challenges in obese patients. Small lesions are generally not well visualized if there is attenuation of the ultrasound beam or X-ray beams. Small lesions in the liver can be masked by the presence of fatty liver which is very common among obese patients. Also, a small renal lesion can be masked by the fat present in the renal hilum. Fatty breast tissue can obscure lesions under the fatty tissue in mammography.
11. Special Challenges in Cardiac Imaging
Diastolic dysfunction is present in all obese patients and is difficult to separate from other pathological causes in an obese patient. Also, most of these patients are hypertensive, and this further complicates the imaging findings. Epicardial fat can also increase the attenuation of ultrasound beams during echocardiography. Also, stress exercises cannot be performed well in obese patients due to difficulty in mobilization. Soft tissue attenuation of radioactive tracers in nuclear cardiology imaging leads to artifacts in imaging.
12. Conclusion
Obese patients face unique challenges in medical imaging and intervention. Over the last few years, medical manufacturers, radiographers, and radiologists have recognized these issues and come up with innovative techniques to overcome these challenges. Pre-trained anesthetists, radiographers, and radiologists in managing obese patients are a prerequisite for treating these patients (Table 1).
| Modalities | Challenges | Solutions |
| Radiograph | •Increased X-ray attenuation •Dose creep •Difficult patient positioning •Difficulty in locating bony landmarks. •Difficulty in achieving coverage of anatomical area | •Using Bucky grid •Double exposure •Increasing tube voltage •Increasing film development speed •Automatic exposure control •Adjusting window level |
| Fluoroscopy | •Weight limit of fluoroscopy table •Inadequate rotation due to motor overload | •Manufacturing heavier special fluoroscopy tables with stronger motor for rotation |
| Mammography | •Increased noise •Decreased image contrast •Motion unsharpness •Difficulty compressing large breasts | •Increasing dose |
| Sonography | •Increased distance of organs from the probe • Increased attenuation of ultrasound waves | •Using low-frequency transducers to increase penetration •Pushing in transducers to decrease the depth of adipose tissue •Placing transducers at the closest distance to the organ of interest •Sound speed correction •Tissue aberration correction technology |
| CT scan | •Gantry size limit •Difficult access for IV lines for contrast injection | •Large gantry •Hula hoop to check diameters •Increased table width and length •Using multiple tourniquets and warm compresses during IV access |
| MRI scan | •Gantry size limit •Space for accommodating phased array coils •Limited FOV •Wrap around artifacts •Skin burns due to skin touching gantry and due to sweat | •Open magnet MRI •Virtual eFOV •Cotton clothes and covering for sweaty arms •Saturation bands |
| NM/PET scan | • Weight-based nuclear medicine dose limits •Insulin causes false negative muscle uptake •Requirement of the pressman fasting state | •Increase FDG dose •Increased data acquisition protocols |
| Interventional radiology | •Difficult vascular access •Difficult visualization of target areas •Inadequate instrument lengths •Increased weight-based radiation dose •Increased anesthesia for patient sedation •Oversedation and under sedation •Delayed post-op recovery •Decreased healing of incision sites •Respiratory compromise in the prone position •Increased risk of pulmonary and deep venous thrombosis | •Using multiple tourniquets and warm compresses during IV access •Manufacturing longer instrument •Special anesthetists training •Technician and radiologist training regarding obesity management |
Table 1: Modality-specific challenges and solutions for obese patients- a summary.
Funding
The author declares that no funds, grants, or other support were received during the preparation of this manuscript.
Competing Interests
The author has no relevant financial or non-financial interests to disclose.
Authors’ Contributions
SSB analyzed and interpreted the data, and was a major contributor to writing the manuscript. The author read and approved the final manuscript.
Ethics Approval
This is a review. The Research Ethics Committee has confirmed that no ethical approval is required.
References
- World Health Organization. Obesity and overweight. Geneva: WHO. 2011.
- Kontis V, Mathers CD, Rehm J, et al. Contribution of six risk factors to achieving the 25×25 non-communicable disease mortality reduction target: a modelling study. Lancet. 2014;384(9941):427-37.
- Machann J, Horstmann A, Born M, et al. Diagnostic imaging in obesity. Best Pract Res Clin Endocrinol Metab. 2013;27(2):261-77.
- Uppot RN. Technical challenges of imaging & image-guided interventions in obese patients. Br J Radiol. 2018;91(1089):20170931.
- Seo G, Robinson J, Punch A, et al. Understanding radiographic decision-making when imaging obese patients: A Think-Aloud study. J Med Radiat Sci. 2022;69(1):13-23.
- Alqahtani SJ, Knapp KM. Imaging patients with obesity. J Med Radiation Sci. 2022;69(1):3-4.
- Hunt KA, Sickles EA. Effect of obesity on screening mammography. AJR Am J Roentgenol. 2000;174(5):1251-255.
- Modica MJ, Kanal KM, Gunn ML. The obese emergency patient: imaging challenges and solutions. Radiographics. 2011;31(3):811-23.
- Napolitano D, Chou C-H, McLaughlin G, et al. Sound speed correction in ultrasound imaging. Ultrasonics. 2006;44(Suppl 1):e43-6.
- Hong HS, Han JK, Kim TK, et al. Ultrasonographic evaluation of the gallbladder: comparison of fundamental, tissue harmonic, and pulse inversion harmonic imaging. J Ultrasound Med. 2001;20(1):35-41.
- Rosenthal SJ, Jones PH, Wetzel LH. Phase inversion tissue harmonic sonographic imaging: A clinical utility study. AJR Am J Roentgenol. 2001;176 (6):1393-398.
- Rosenthal K. Selecting the best I.V. site for an obese patient. Nursing. 2004;34(11):14.
- Uppot RN. Impact of obesity on radiology. Radiol Clin North Am. 2007;45(2):231-46.
- European Commission. Criteria for Acceptability of Radiological (including Radiotherapy) and Nuclear Medicine Installation. Radiation Protection No 91, 1997.
- Uppot R, Sheehan A, Seethamraju R. Obesity and MR imaging. In: MRI hot topics 2005. Malvern, PA: Seimens Medical Solutions USA.
- Botkin CD, Osman MM. Prevalence, challenges, and solutions for (18)F-FDG PET studies of obese patients: a technologist’s perspective. J Nucl Med Technol. 2007;35(2):80-83.
- Buckley O, Ward E, Ryan A, et al. European obesity and the radiology department. What can we do to help? Eur Radiol. 2009;19(2):298-309.
