Summary
Blood group antigens are hereditarily determined and play a vital role in blood safety. Blood types are known to have some association with many diseases. About 700 erythrocyte antigens have been described, organized into 30 blood group systems by the International Society of Blood Transfusion, of which the ABO and Rhesus systems are the most important. Thus, knowledge of the distribution of ABO and Rhesus blood groups at the local and/or regional level is of major importance in the management of blood banks and transfusion safety services.
Keywords
distribution; antigen; blood groups and Rhesus; Yangambi
Introduction
Blood group antigens are determined hereditarily and play a vital role in blood safety, population genetics studies, research on the migratory movements of peoples, the phenomenon of heredity, medico-legal problems, cases of disputed paternity, and predisposition to certain diseases [1, 2]. Speaking of diseases, blood types are known to have some association with many diseases like duodenal ulcers, diabetes mellitus, urinary tract infections, Rh incompatibility, and ABO incompatibility in newborns and certain cancers [3–7]. This means that the spectrum of application for the discovery of blood groups by Landsteiner is very broad and covers areas as varied as immunohematology, transfusion between different individuals, incompatible pregnancies, forensic medicine, and anthropology. About 700 red blood cell antigens have been described, organized into 30 blood group systems by the International Society of Blood Transfusion, of which the ABO and Rhesus systems are the most important [2, 8–14]. Thus, knowledge of the distribution of ABO and Rhesus blood groups at the local and/or regional level is of imperative importance in the management of blood banks and transfusion safety services. This constitutes our current concern and research question, given the lack of data on this subject in Yangambi, in the territory of Isangi in the Democratic Republic of Congo.
The objectives pursued are first to improve the management of the blood bank and the transfusion safety service and then to determine the frequency of ABO and Rhesus blood groups among voluntary blood donors monitored at the Yangambi Blood Transfusion Center. Also, to determine the distribution of ABO and Rhesus blood groups among the blood donors followed according to age and sex.
Materials and Methods
Material
This study was conducted at the INERA Yangambi Reference General Hospital, which is a blood transfusion center.
Our study involved blood donors aged 18–55 who resided in Yangambi and agreed to give their blood voluntarily. The criteria for inclusion in the study were as follows:
a) Clinical criteria
- Having consulted the center for transfusion safety during the period from January 1, 2021 to December 31, 2021;
- Have fully undergone the screening examination before donating blood;
- Be a donor and have given informed consent;
- Have an individual selection form completed correctly;
- Be between 18 and 55 years old;
- Have a minimum weight of 50 kg;
- Have a systolic blood pressure between 120- and 140 mmHg;
- Have no clinical signs that could contraindicate a blood donation.
b) Biological criteria
- Have a hemoglobin level – Male: Hb ≥12 g/dL; Female: Hb≥11 g/dL.
Were excluded from this study, donors with an incomplete protocol sheet.
The study thus focused on 99 blood donors of two sexes. These candidates have never been transfused.
- A sphygmomanometer, a double cup stethoscope, a wristwatch;
- A bathroom scale with height rod, a country bed;
- Pairs of scissors, a tourniquet, alcohol, lancet, adhesive plaster, temporary tube, hemolysis tube, transfer pipette, rack;
- Rhesoscope to visualize fine agglutination, centrifuge, incubator;
- A donor selection sheet, blood and serum samples;
- Reagents: anti-A serum (blue), anti-B serum (yellow), anti-AB serum (clear, colorless), anti-D serum (colorless).
Methods
This is a descriptive, cross-sectional study carried out from January 1 to December 31, 2021.
- Principle of blood grouping according to Beth Vincent
The determination of an ABO blood group involves two tests: a globular test (known as Beth Vincent) which makes it possible to search for the antigens carried by the red blood cells of the subject tested using anti-A and anti-B antiserum, and a serum test (known as Simonin) which demonstrates the antibodies present in the serum using red blood cells of known phenotype.
At the INERA Yangambi General Reference Hospital, blood grouping according to Beth Vincent is used, the principle of which is shown in the table below (Table 1). If a realization is positive with them, one should look for irregular antibodies and if possible, identify them with an identification panel.
Beth Vincent globular test |
| Detection of erythrocyte antigens | Results |
| Test serums |
| Anti-A | Anti-B | Anti-AB | Group |
| +++ | ─ | +++ | A |
| ─ | +++ | +++ | B |
| ─ | ─ | ─ | AB |
| +++ | +++ | +++ | O |
Table 1: Beth Vincent blood grouping.
- Procedure for blood group determination
- Wash the red blood cells and prepare the 10% suspension, e., 1 volume of the pellet;
- after washing, plus 9 volumes of physiological water;
- Properly arrange the materials;
- Group: place a drop of anti-A serum in the first well, another anti-B in the second well, another anti-AB in the third well, and the last well put anti-D;
- Add a drop of suspension in the four different wells;
- Mix; do the reading.
Interpretation: Read after 5 seconds. If there is agglutination in cup A, AB, and D, the person is group A rhesus positive; if there is agglutination in B, AB, and D, the person is group B rhesus positive.
The interview specified the socio-demographic characteristics of the donors, in particular age, sex, and occupation.
- Data processing and analysis
Data was collected from the hospital’s blood donor registers and files. After data collection, we also carried out quality checks and manual counting. The results were described in terms of proportions for the categorical variables. The main results we obtained have been presented in the form of tables.
Results
Sociodemographic characteristics of the respondents
Table 2 and Figure 1 presents the sociodemographic characteristics of the blood donors in our survey. Table 2 shows that the majority of respondents, i.e., 52.53%, were between 18 and 24 years old.
| Age | Effective | Percentage |
| 18–24 | 52 | 52.53% |
| 25–29 | 25 | 25.25% |
| 30–34 | 11 | 11.11% |
| 35–39 | 4 | 4.04% |
| 40–44 | 3 | 3.03% |
| 45–49 | 2 | 2.02% |
| ≥50 | 2 | 2.02% |
Table 2: Age.
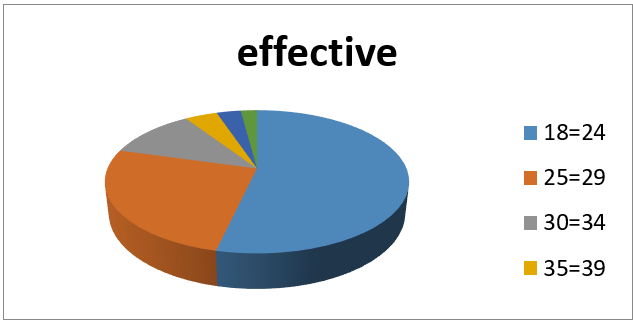
Figure 1: Breakdown by age.
Table 3 and Figure 2 shows that 98% of blood donors were men, and 2% were women.
| Sex | Effective | Percentage |
| Men | 97 | 98% |
| Women | 2 | 2% |
Table 3: Sex.
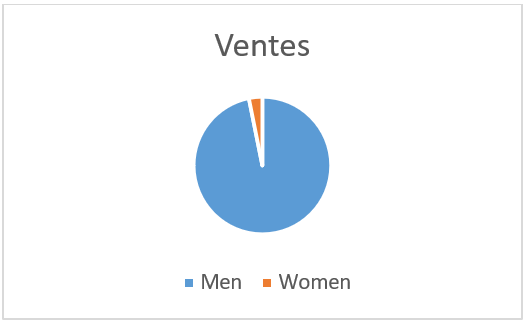 Figure 2: Breakdown by sex.
Figure 2: Breakdown by sex.
Table 4 and Figure 3 shows that pupils and students represented the largest segment with 39.4%, followed by all-work agents with 29.3% and the unemployed with 25.3%.
| Profession | Effective | Percentage |
| Pupils/students | 39 | 39.4% |
| All jobs | 29 | 29.3% |
| Unemployed | 25 | 25.3% |
| Salaried workers | 5 | 5% |
| Tradespeople | 1 | 1% |
Table 4: Profession.
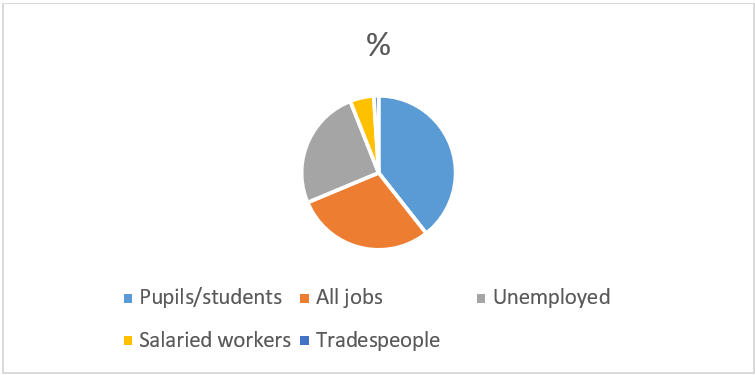 Figure 3: Profession.
Figure 3: Profession.
Table 5 shows the frequency of blood groups among blood donors.
| A+ | A- | B+ | B- | AB+ | AB- | O+ | O- | Total |
26
(26.3%) | 0
(0%) | 17
(17.2%) | 1
(1%) | 5
(5%) | 0
(0%) | 49
(49.5%) | 1
(1%) | 99
(100%) |
Table 5: Frequency of blood groups.
According to the results in Table 5, the most frequent blood group was group O+ (49.5%), followed by group A+ (26.3%), B+ (17.2%), and finally AB+ (5%). We recorded two cases of the Rhesus negative group: 1B- (1%) and 1O- (1%).
Distribution of blood groups according to age
Table 6 shows the distribution of blood groups according to age.
| Age (years) | A N(%) | B N(%) | AB N(%) | O N(%) | Total N(%) |
| 18–24 | 11(21.2%) | 10(19.2%) | 5(9.6%) | 26(50%) | 52(100%) |
| 25–29 | 8(36%) | 4(16%) | 0(0%) | 12(48%) | 25(100%) |
| 30–34 | 4(36.5%) | 2(19%) | 0(0%) | 5(45.5%) | 11(100%) |
| 35–39 | 1(25%) | 1(25%) | 0(0%) | 2(50%) | 4(100%) |
| 40–44 | 1(33.3%) | 0(0%) | 0(0%) | 2(66,7%) | 3(100%) |
| 45–49 | 0(0%) | 1(50%) | 0(0%) | 1(50%) | 2(100%) |
| ≥50 | 1(50%) | 0(0%) | 0(0%) | 1(50%) | 2(100%) |
| Total | 26 | 18 | 5 | 50 | 99 |
Table 6: Distribution of blood groups by age.
The distribution of blood groups according to age (Table 6) shows the following:
- Blood group O was more frequent in all sections.
- Blood group A was more common in the 30–34 age group (36.5%), 25–29 years old (36%), and 40–44 years old (33.3%).
- Blood group B was more frequent in the age groups 35–39 years old (25%), followed by the age group 18– 24 years old (19.2%) and 30–34 years old (19%).
Distribution of blood groups according to sex
Table 7 shows the distribution of blood groups of voluntary donors according to sex.
| Sex | A+ | A- | B+ | B- | AB+ | AB- | O+ | O- | Total |
| Men | 26 (26.8%) | 0 (0%) | 17 (17.5%) | 1 (2.1%) | 4 (4.1%) | 0 (0%) | 48 (49.5%) | 1 (2.1%) | 97 (100%) |
| Women | 0 | 0 | 0 | 0 | 1 (50%) | 0 | 1 (50%) | 0 | 2 (100%) |
| Total | 26 (26.3%) | 0 | 17 (17.2%) | 1 (1%) | 5 (5%) | 0 | 49 (49.5%) | 1 (1%) | 99 (100%) |
Table 7: Distribution of blood groups by sex.
Distribution of blood groups in the male sex reflects the overall pattern: 95 Rhesus positive and 2 Rhesus negative men, with O+, A+, B+, AB+, B- and O- in order of frequency. Two women in our series were Rhesus positive.
Distribution of blood groups according to occupation
Table 8 shows the distribution of blood groups according to occupation.
| Profession | A N(%) | B N(%) | AB N(%) | O N(%) | Total N(%) |
| Pupils/students | 8(20.5%) | 7(18%) | 4(10.2%) | 20(51.3%) | 39(100%) |
| All work | 10(34.5%) | 5(17.2%) | 0 | 14(48.3%) | 29(100%) |
| Unemployed | 7(28%) | 4(16%) | 0 | 14(56%) | 25(100%) |
| Salaried workers | 1(20%) | 2(40%) | 0 | 2(40%) | 5(100%) |
| Tradesmen | 0 | 0 | 1(100%) | 0 | 1(100%) |
| Total | 26 | 18 | 5 | 50 | 99 |
Table 8: Distribution of blood groups according to profession.
Table 8 relating to the distribution of groups blood tests according to profession reveals that the proportion of group O was higher among the unemployed (56%), followed by that of pupils/students (51.3%). The proportion of group A was the highest among all-work subjects (34.5%), and for group B, the proportion is higher among salaried workers (40%).
Discussion
Overall frequency of blood groups
In our series, the order of frequency of blood groups in the ABO system was as follows: O+, A+, B+, and AB+ (Table 5). In France, the most common blood type was group A (45%), followed by groups O (43%), B (9%), and AB (3%), according to the French Blood Establishment. In the ABO system, the work of Singh et al. in India showed, among blood donors, a high frequency of blood group B (35.15%), followed by O (34.73%), A (22.09%), and AB (8.03%) [1]. With regard to the Rhesus negative group, it was only identified with us in two cases, i.e., 2%: 1B- and 1O-. In France, the French Blood Establishment provided the following results: A- 7%, O- 6%, B- 1%, AB-1%, or 15% in total. In India, Singh et al. mentioned, for the year 2015, 3.6% of Rhesus negative donors against 96.4% of Rhesus positive [1].
The figures mentioned in the series of Singh et al. [1] show differences sometimes enormous, for example, the frequency of blood group O in Pakistan and India compared to Nigeria and at home in Yangambi. This could be explained by the very small number of our sample recruited from elsewhere during one year.
However, a child’s blood type is based on that of their parents. It is indeed defined in relation to the group of its parents, which is based on two alleles. Each individual receives two A, B, or O alleles. The A and B alleles are dominant, and the O allele is recessive: the latter can only be expressed in the presence of a second O allele. A child with blood group A may have inherited one A allele, one O allele, or two A alleles. A child with blood group B may have inherited one B allele, one O allele, or two B alleles. For group AB, it is necessary to have the allele A and the allele B (co-dominant). The subjects of the group O obligatorily received two alleles O [9, 11].
Sociodemographic characteristics and blood donation
Among the donors who attended the INERA Yangambi General Reference Hospital, there were more men than women, more young people than elderly people, and almost 40% pupils and students (Table 3).
- Age
Several African studies have shown that blood donors in Africa are often young. In Kenya, Rajab et al. reported a mean age of 28.9 ± 8.5 years among their blood donors [15]; in Rwanda, Tagny et al. observed that more than 75% of blood donors were under 30 years old [16]. These average ages observed in Africa are 10–15 years lower than those observed in European countries, particularly in France, Belgium, and the United Kingdom, where the proportion of donors under 35 was less than 50% and less than 45% in Switzerland and Finland [17]. The difference can be explained by the fact that blood donation programs in Africa are aimed primarily at secondary school students and university students whose average age varies between 18 and 25 years. - Sex
Concerning women’s participation in blood donation, we believe that several factors probably constituted a significant barrier to blood donation among women in the city of Yangambi, in particular fear, fragile health, numerous deliveries, culture, poverty, ignorance, and religion. This phenomenon has also been found in other poor countries in India and Africa, with the proportion of women among blood donors being low: 8.27% for Singh et al. in India [1]; in Africa, Tagny et al. [16] found the following proportions: 30% in Togo, 10% in Ghana, 9.9% in Nigeria. In these countries, this may be due to socio-cultural reasons, lack of motivation and fear of getting sick and dying [18], and sometimes discouragement of female donors. - Profession
Concerning the profession, apart from the pupils and students because of their age and education, we think the differences observed were purely descriptive and could be the subject of further in-depth studies.
Conclusion
Knowledge of blood group distribution is very important for blood banks and blood transfusion services as they play a significant role in patient health care. This study showed that a particular group of subjects (women) did not seem to adhere to the blood donation policy. This group should be encouraged to give blood more frequently. Each individual should be grouped. This can be of enormous use in the event of acute haemorrhage, anemia of the child, or a transfusion emergency at the time of childbirth.
References
- Singh A, Srivastava RK, Deogharia KS, et al. Distribution of ABO and Rh types in voluntary Blood donors in Jharkhand area as a study conducted by RIMS, Ranchi. J Family Med Prim Care. 2016;5(3):631-36.
- Jolly JG. Medicolegal significance of human blood groups. J Indian Med Assoc. 2000;98(6):340-41.
- Mehta N, Swadas B. Prevalence of ABO blood groups at Mahavir Heart Institute Surat. Asian J Trans Sci. 2012;6(1):74-75.
- Khan MI, Micheal S, Akhtar F, et al. Association of ABO blood groups with glaucoma in the Pakistani population. Can J Ophthalmol. 2009;44(5):582-86.
- Xie J, Qureshi AA, Li Y, et al. ABO blood group and incidence of skin cancer. PLoS One. 2010;5(8):e11972.
- Amundadottir L, Kraft P, Stolzenberg-Solomon RZ, et al. Genome-wide association study identifies variants in the ABO locus associated with susceptibility to pancreatic cancer. Nat Genet. 2009;41(9):986-90.
- Gates MA, Wolpin BM, Cramer DW, et al. ABO blood group and incidence of epithelial ovarian cancer. Int J Cancer. 2011;128(2):482-86.
- Dzieczkowski JS, Anderson KC. Biologie de la transfusion et thérapeutique transfusionnelle. In : Kasper DL, Braunwald E, Fauci AS, et al (eds). Harrison Principes de Médecine Interne, 16è éd. Paris: Flammarion Médecine Sciences; 2006.
- Marieb EN, Hoehn K. Anatomie et physiologie humaines. Nouveaux Horizons, Paris: ARS; 2015.
- Lefrère JJ, Berche P. Karl Landsteiner découvre les groupes sanguins. Transfus Clin Biol. 2010;17(1):1-8.
- Brecher ME. Traitement par des dérivés sanguins. In : Runge MS, Greganti MA, eds : Médecine Interne de Netter. 2ème édition, Elsevier Masson ; Paris ; 2011.
- Sherwood L. Physiologie humaine. 2nd éd. De Boeck. Paris: Nouveaux Horisons – ARS; 2010.
- Salomon BA, Bernard MM, Lucien BB, et al. Blood Group Phenotype Frequencies in Blood Donors in the Northeast of Democratic Republic of Congo. Int blood res rev. 2017;7(2):1-5.
- Barritt AS, Fried MW. Hépatite virale : maladie aiguë er chronique. In : Runge MS, Greganti MA, (eds). Médecine Interne de Netter, 2nd éd. Paris: Elsevier Masson; 2011.
- Rajab JA, Muchina WP, Orinda DA, et al. Blood donor haematology parameters in two regions of Kenya. East Afr Med J. 2005;82(3):123-27.
- Tagny CT, Owusu-Ofori S, Mbanya D, et al. The blood donor in sub-Saharan Africa: a review. Transfus Med. 2010;20(1):1-10.
- Lefr`ere, JJ, Rouger P. Pratique Nouvelle de laTransfusion Sanguine, 2nd éd. Paris: Masson; 2006.
- Batina-Agasa S, Kambale-Kombi P, Kabamba P, et al. Sickle cell trait among blood donors in the Democratic Republic of the Congo: which transfusion policy for Sickle cell patients? ISBT Sci Ser. 2021;16(1):56-59.
